

Association of lower costs of pulsatile machine perfusion in renal transplantation from expanded criteria donors
- PMID: 18925906
- PMCID: PMC2596761
- DOI: 10.1111/j.1600-6143.2008.02412.x
Association of lower costs of pulsatile machine perfusion in renal transplantation from expanded criteria donors
Abstract
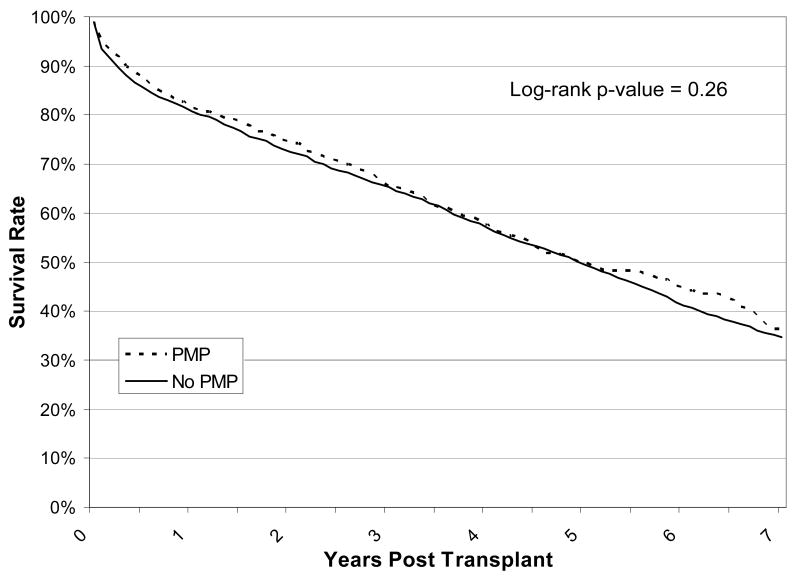
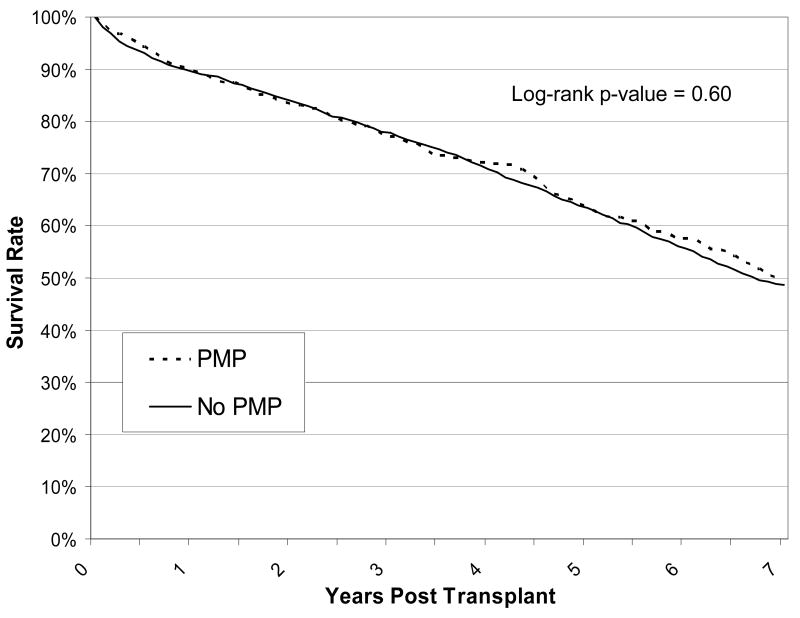
Pulsatile machine perfusion (PMP) has been shown to reduce delayed graft function (DGF) in expanded criteria donor (ECD) kidneys. Here, we investigate whether there is a cost benefit associated with PMP utilization in ECD kidney transplants. We analyzed United States Renal Data System (USRDS) data describing Medicare-insured ECD kidney transplant recipients in 1995-2004 (N = 5840). We examined total Medicare payments for transplant hospitalization and annually for 3 years posttransplant according to PMP utilization. After adjusting for other recipient, donor and transplant factors, PMP utilization was associated with a $2130 reduction (p = 0.007) in hospitalization costs. PMP utilization was also associated with lower DGF risk (p < 0.0001). PMP utilization did not predict differences in rejection, graft survival, patient survival, or costs at 1, 2 and 3 years posttransplant. PMP utilization is correlated with lower costs for the transplant hospitalization, which is likely due to the associated reduction in DGF among recipients of PMP kidneys. However, there is no difference in long-term Medicare costs for ECD recipients by PMP utilization. A prospective trial is necessary as it will help determine if the associations seen here are due to PMP utilization and not differences in the population studied.
Figures
Similar articles
-
Economic impact of the introduction of machine perfusion preservation in a kidney transplantation program in the expanded donor era: cost-effectiveness assessment.Transplant Proc. 2012 Nov;44(9):2521-4. doi: 10.1016/j.transproceed.2012.09.065. Transplant Proc. 2012. PMID: 23146442
-
Pulsatile perfusion reduces the incidence of delayed graft function in expanded criteria donor kidney transplantation.Am J Transplant. 2006 Jun;6(6):1473-8. doi: 10.1111/j.1600-6143.2006.01323.x. Am J Transplant. 2006. PMID: 16686773
-
Evaluation of quality of kidneys from donation after circulatory death/expanded criteria donors by parameters of machine perfusion.Nephrology (Carlton). 2018 Feb;23(2):103-106. doi: 10.1111/nep.12971. Nephrology (Carlton). 2018. PMID: 27888556
-
Machine perfusion preservation versus static cold storage for deceased donor kidney transplantation.Cochrane Database Syst Rev. 2019 Mar 15;3(3):CD011671. doi: 10.1002/14651858.CD011671.pub2. Cochrane Database Syst Rev. 2019. Update in: Cochrane Database Syst Rev. 2024 Jul 9;7:CD011671. doi: 10.1002/14651858.CD011671.pub3. PMID: 30875082 Free PMC article. Updated.
-
The clinical and cost-effectiveness of pulsatile machine perfusion versus cold storage of kidneys for transplantation retrieved from heart-beating and non-heart-beating donors.Health Technol Assess. 2003;7(25):1-94. doi: 10.3310/hta7250. Health Technol Assess. 2003. PMID: 14499050 Review.
Cited by
-
Case mix, quality and high-cost kidney transplant patients.Am J Transplant. 2009 May;9(5):1108-14. doi: 10.1111/j.1600-6143.2009.02592.x. Am J Transplant. 2009. PMID: 19422336 Free PMC article.
-
Maximizing kidneys for transplantation using machine perfusion: from the past to the future: A comprehensive systematic review and meta-analysis.Medicine (Baltimore). 2016 Oct;95(40):e5083. doi: 10.1097/MD.0000000000005083. Medicine (Baltimore). 2016. PMID: 27749583 Free PMC article.
-
Kidney transplant Medicare payments and length of stay: associations with comorbidities and organ quality.Arch Med Sci. 2011 Apr;7(2):278-86. doi: 10.5114/aoms.2011.22079. Epub 2011 May 17. Arch Med Sci. 2011. PMID: 22291768 Free PMC article.
-
The Changing Financial Landscape of Renal Transplant Practice: A National Cohort Analysis.Am J Transplant. 2017 Feb;17(2):377-389. doi: 10.1111/ajt.14018. Epub 2016 Oct 4. Am J Transplant. 2017. PMID: 27565133 Free PMC article.
-
Hypothermic machine perfusion reduces delayed graft function and improves one-year graft survival of kidneys from expanded criteria donors: a meta-analysis.PLoS One. 2013 Dec 10;8(12):e81826. doi: 10.1371/journal.pone.0081826. eCollection 2013. PLoS One. 2013. PMID: 24339970 Free PMC article. Review.
References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LYC, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. The New England Journal of Medicine. 1999;341(23):1725–1730. - PubMed
-
- Ojo AO, Hanson JA, Meier-Kriesche HU, Okechukwu CN, Wolfe RA, Leichtman AB, et al. Survival in recipients of marginal cadaveric donor kidneys compared with other recipients and wait-listed transplant candidates. Journal of the American Society of Nephrology. 2001;12(3):589–597. - PubMed
-
- Matas AJ, Schnitzler MA. Payment for living donor (vendor) kidneys: a cost-effectiveness analysis. American Journal of Transplantation. 2004;4(2):216–221. - PubMed
-
- Andreoni KA, Brayman KL, Guidinger MK, Sommers CM, Sung RS. Kidney and pancreas transplantation in the United States, 1996-2005. American Journal of Transplantation. 2007;7(5 Pt 2):1359–1375. - PubMed
-
- Peter SD, Imber CJ, Friend PJ. Liver and kidney perservation by perfusion. The Lancet. 2002;359:604–613. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
