

2202 kidney transplant recipients with 10 years of graft function: what happens next?
- PMID: 18925907
- PMCID: PMC2766174
- DOI: 10.1111/j.1600-6143.2008.02414.x
2202 kidney transplant recipients with 10 years of graft function: what happens next?
Abstract
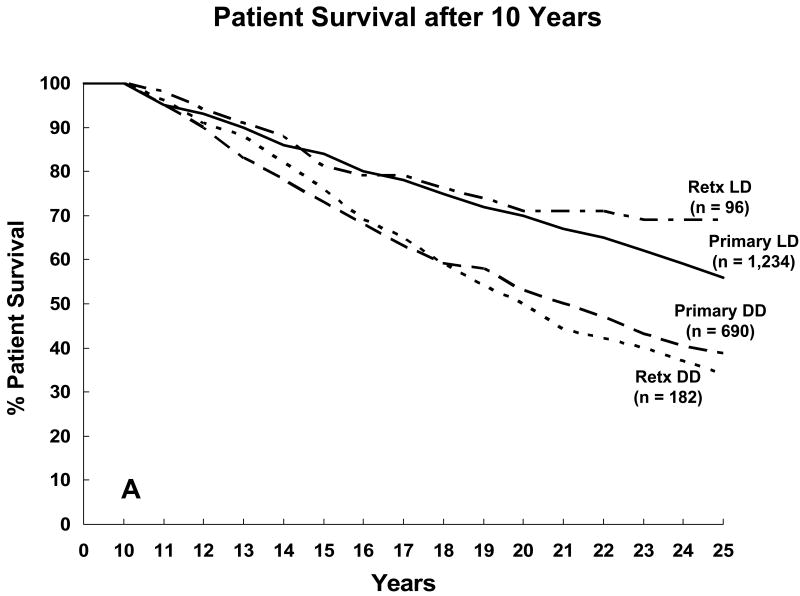
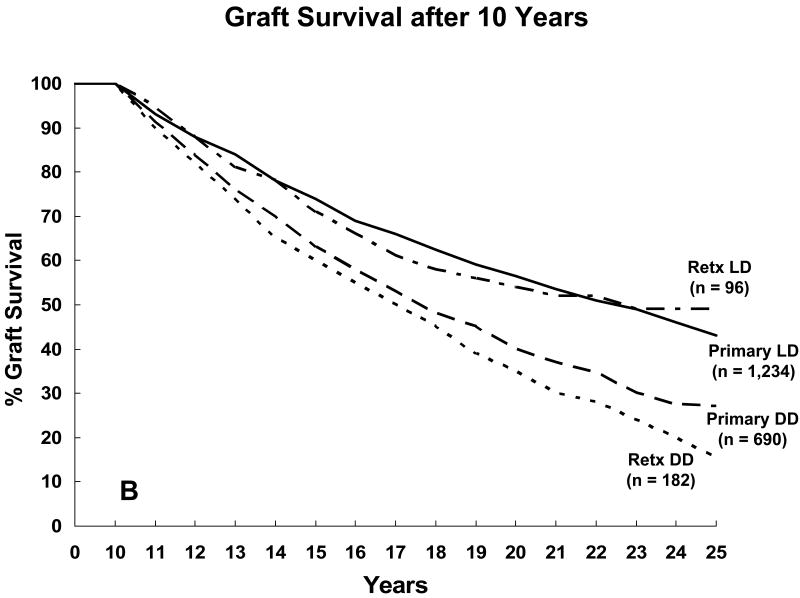
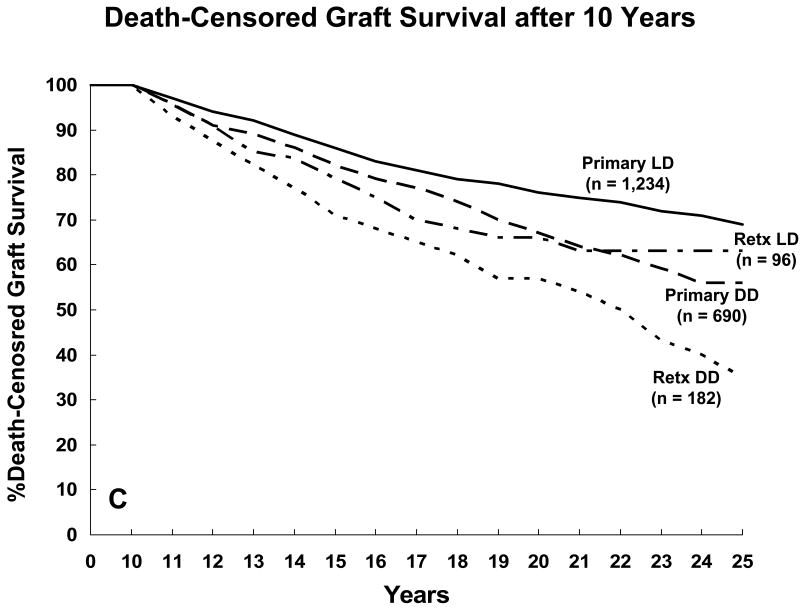
The ultimate goal of clinical transplantation is for the recipients to achieve long-term survival, with continuing graft function, that is equivalent to that of the age-matched general population. We studied subsequent outcome in kidney transplant recipients with 10 years of graft function. In all, 2202 kidney transplant recipients survived with graft function >10 years. For 10-year survivors, the actuarial 25-year patient survival rate for primary transplant living donor (LD) recipients was 57%; graft survival, 43%. For primary transplant deceased donor (DD) recipients, the actuarial 25-year patient survival rate was 39%; graft survival, 27%. The two major causes of late graft loss were death (with graft function) and chronic allograft nephropathy (tubular atrophy and interstitial fibrosis). The two major causes of death with function were cardiovascular disease (CVD) and malignancy. For nondiabetic recipients, the mean age at death with function from CVD was 54 +/- 13 years; for diabetic recipients, 53 +/- 7 years. By 20 years posttransplant, morbidity was common: >40% recipients had skin cancer (mean age for nondiabetic recipients, 53 +/- 13 years; for diabetics, 49 +/- 8 years), >10% had non-skin cancer (mean age for nondiabetic recipients, 53 +/- 16 years; for diabetics, 46 +/- 9 years), and >30% had CVD (mean age for nondiabetic recipients, 53 +/- 15 years; for diabetics, 47 +/- 9 years). We conclude that long-term transplant recipients have a high rate of morbidity and early mortality. As short-term results have improved, more focus is needed on long-term outcome.
Figures
References
-
- Wolfe RA, Ashby VB, Mitford EL, Ojo AO, Ettenger RE, Agodoa LYC, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341:1725–1730. - PubMed
-
- Evans RW, Manninen DL, Garrison LP, Jr, Hart LG, Blagg DR, Gutman RA, et al. The quality of life of patients with end-stage renal disease. N Engl J Med. 1985;312(9):553–9. - PubMed
-
- Meier-Kriesche HU, Baliga R, Kaplan B. Decreased renal function is a strong risk factor for cardiovascular death after renal transplantation. Transplantation. 2003;75(8):1291–5. - PubMed
-
- Matas AJ, Sutherland DE, Najarian JS. Evolution of immunosuppression at the University of Minnesota. Transplant Proc. 2004;36(2 Suppl):64S–70S. - PubMed
-
- Dunn DL, Gillingham KJ, Kramer MA, Schmidt WJ, Erice A, Balfour HH, Jr, et al. A prospective randomized study of acyclovir versus gangiclovir plus human immune globulin prophylaxis of cytomegalovirus infection after solid organ transplantation. Transplantation. 1994;57(6):876–84. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
