

High-resolution imaging in Barrett's esophagus: a novel, low-cost endoscopic microscope
- PMID: 18926182
- PMCID: PMC2869299
- DOI: 10.1016/j.gie.2008.05.018
High-resolution imaging in Barrett's esophagus: a novel, low-cost endoscopic microscope
Abstract
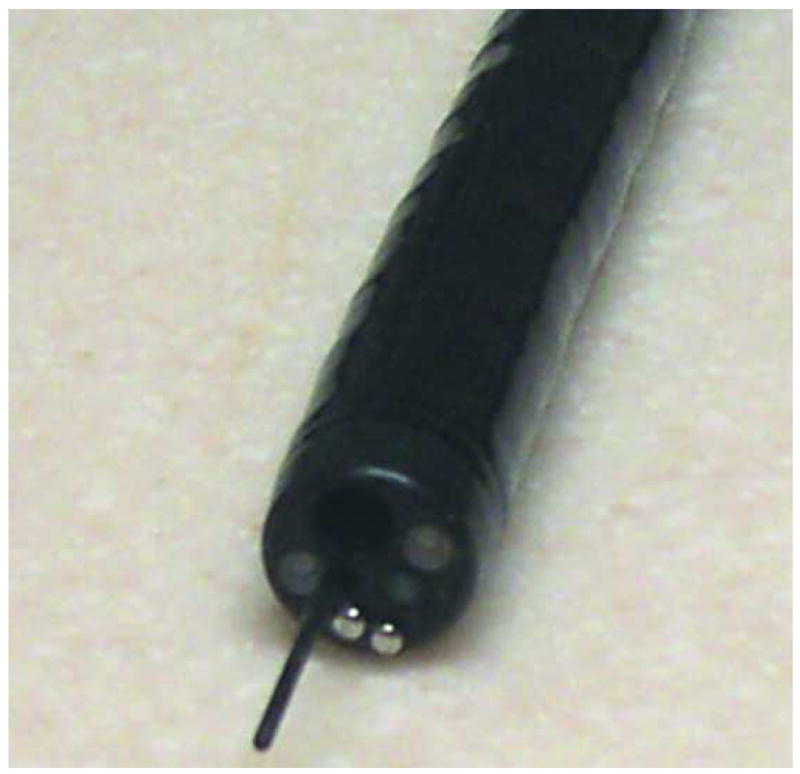
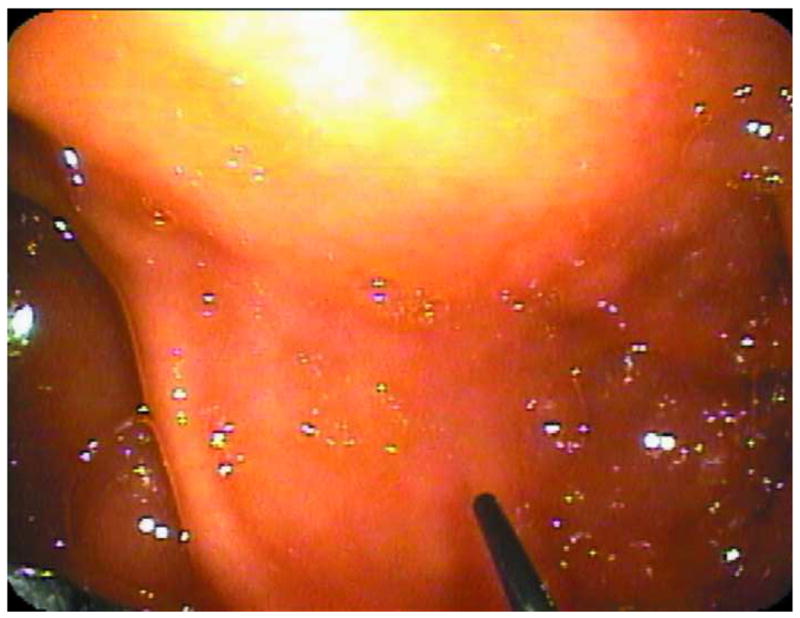
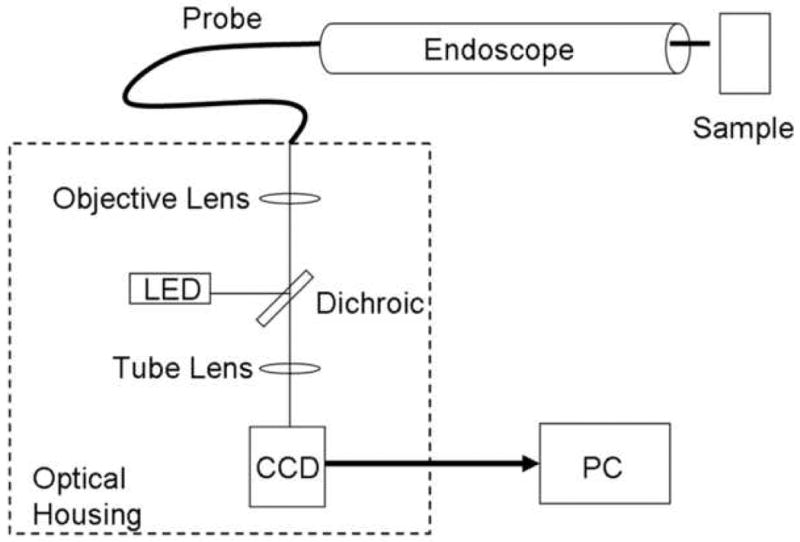
Background: This report describes the clinical evaluation of a novel, low-cost, high-resolution endoscopic microscope for obtaining fluorescent images of the cellular morphology of the epithelium of regions of the esophagus with Barrett's metaplasia. This noninvasive point imaging system offers a method for obtaining real-time histologic information during endoscopy.
Objective: The objective of this study was to compare images taken with the fiberoptic endoscopic microscope with standard histopathologic examination.
Design: Feasibility study.
Setting: The University of Texas M.D. Anderson Cancer Center Department of Gastroenterology. PATIENTS, INTERVENTIONS, AND MAIN OUTCOME MEASUREMENTS: The tissue samples studied in this report were obtained by endoscopic resection from patients with previous diagnoses of either high-grade dysplasia or esophageal adenocarcinoma.
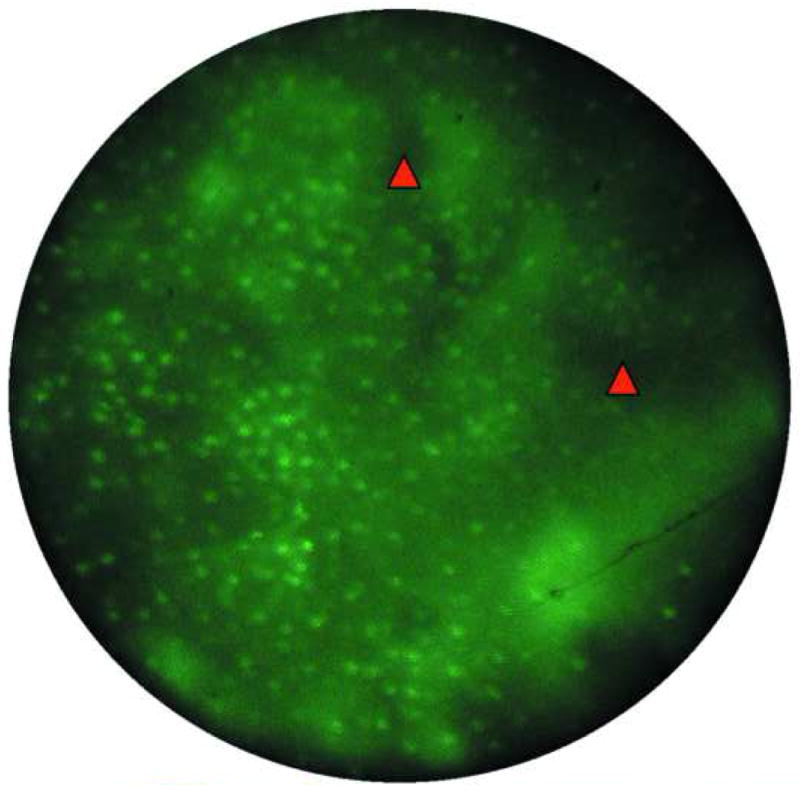
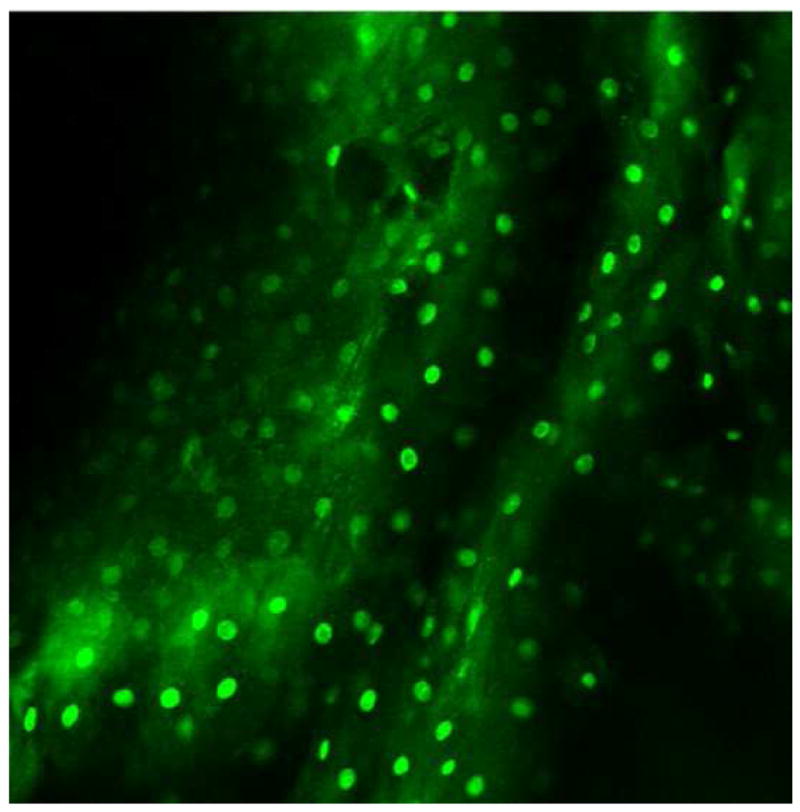
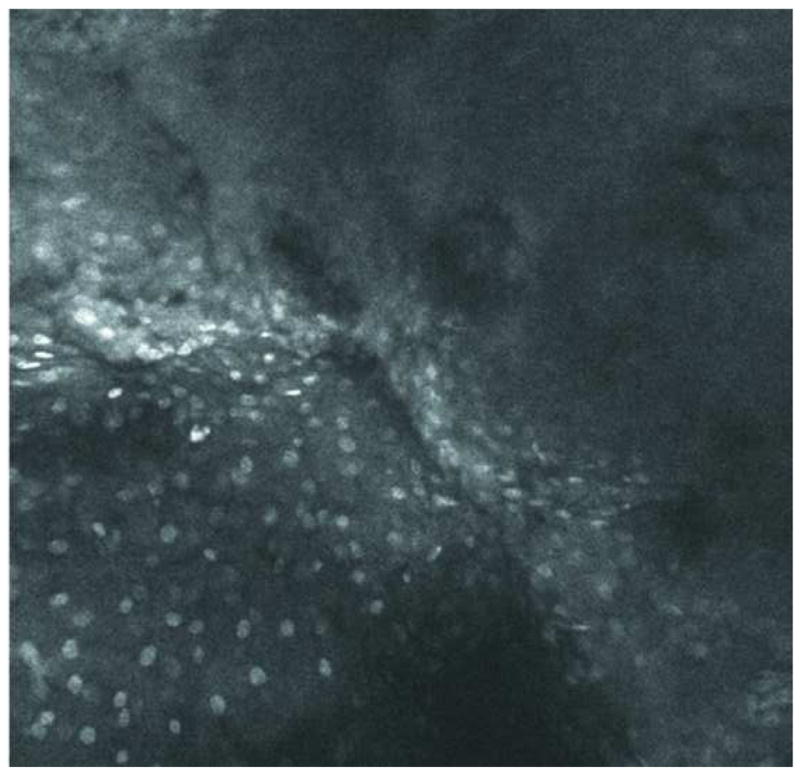
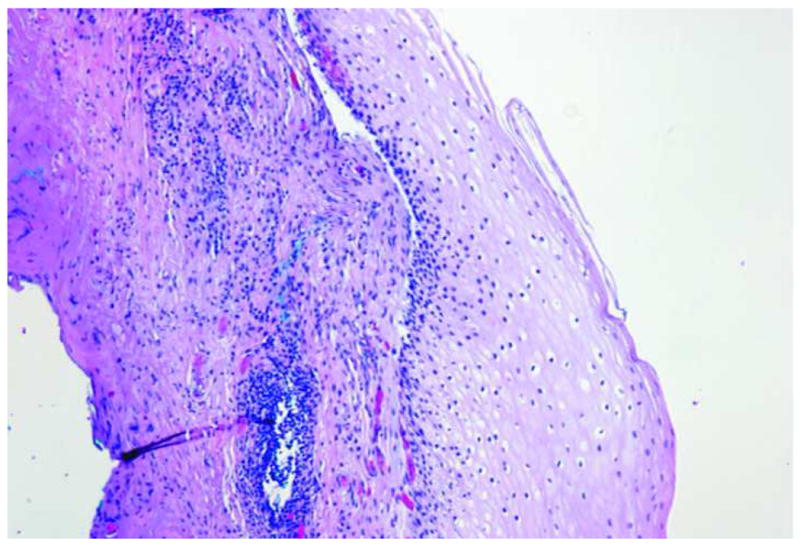
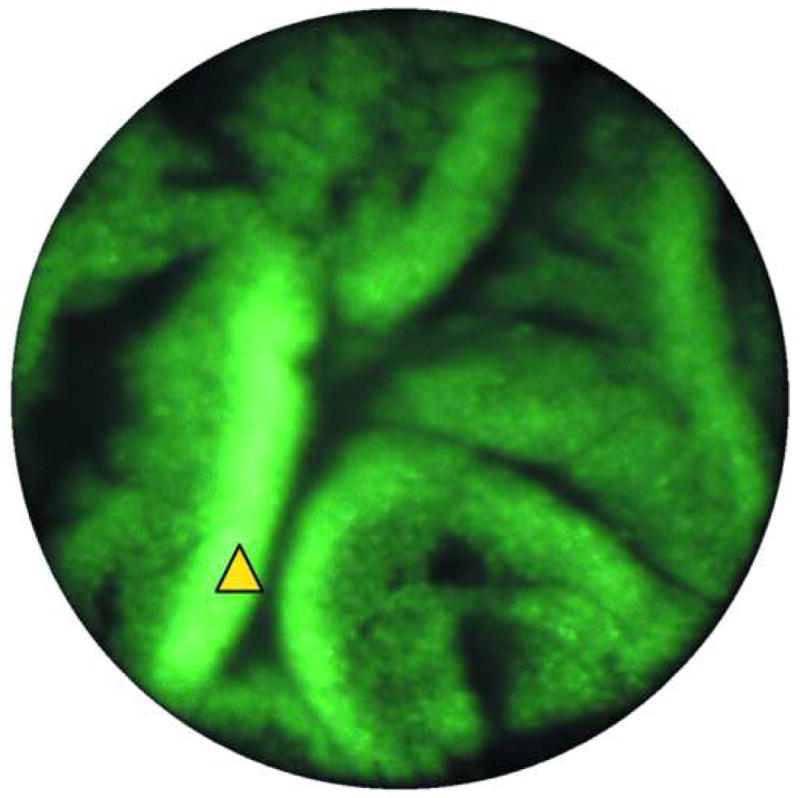
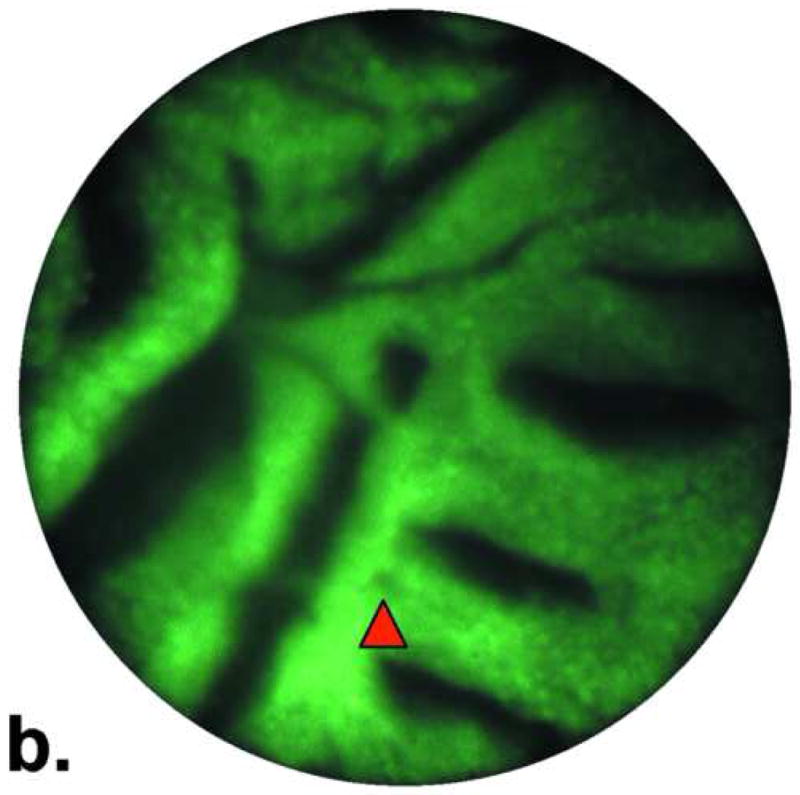
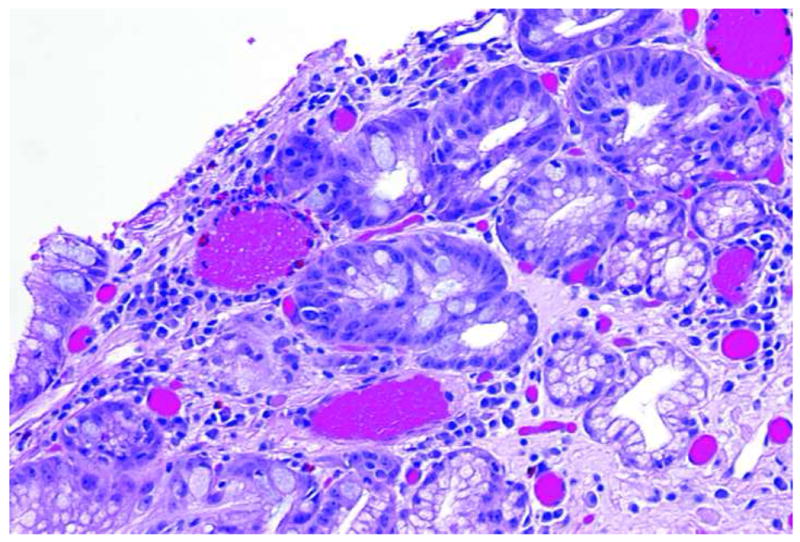
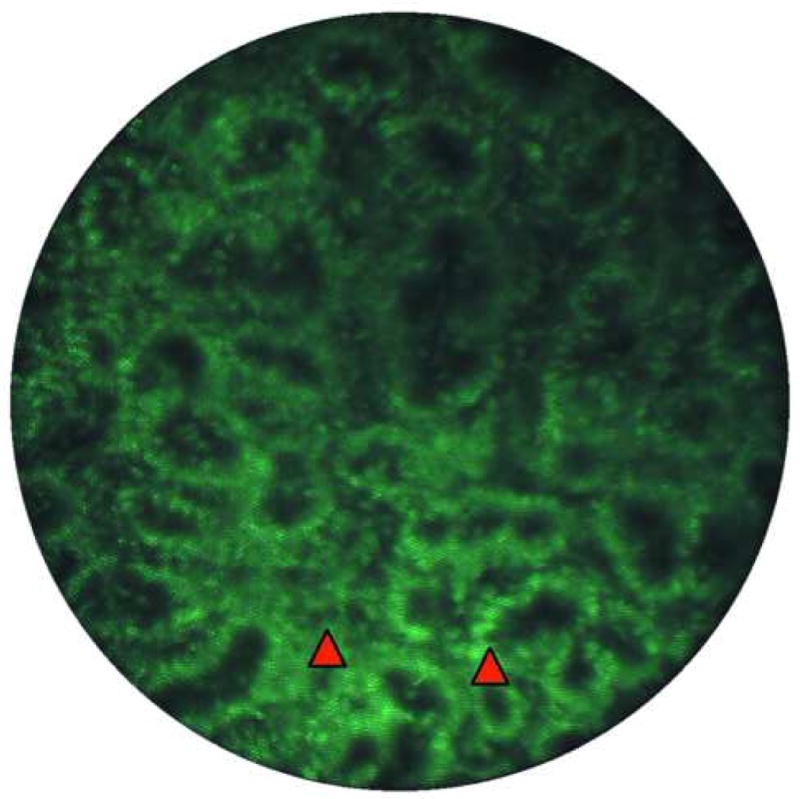
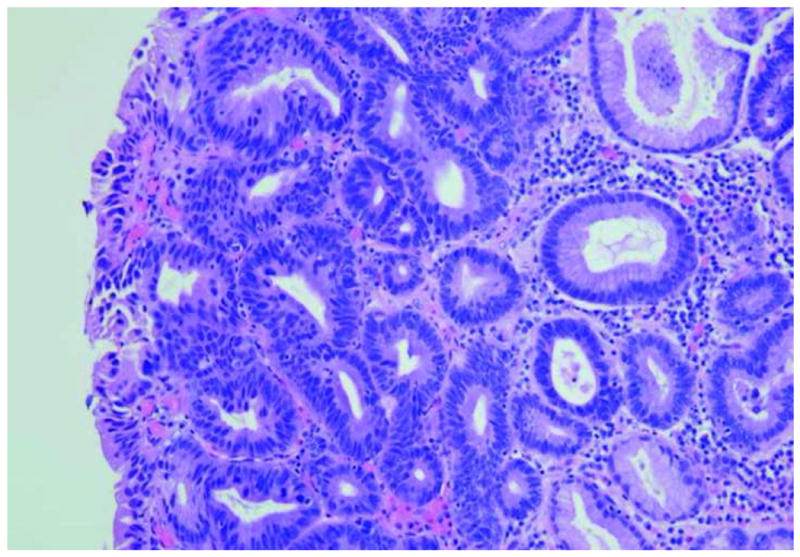
Results: Three distinct tissue types were observed ex vivo with the endoscopic microscope: normal squamous mucosa, Barrett's metaplasia, and high-grade dysplasia. Squamous tissue was identified by bright nuclei surrounded by dark cytoplasm in an ordered pattern. Barrett's metaplasia could be identified by large glandular structures with intact nuclear polarity. High-grade dysplasia was visualized as plentiful, irregular glandular structures and loss of nuclear polarity. Standard histopathologic examination of study samples confirmed the results obtained by the endoscopic microscope.
Limitations: The endoscopic microscope probe had to be placed into direct contact with tissue.
Conclusions: It was feasible to obtain high-resolution histopathologic information using the endoscopic microscope device. Future improvement and integration with widefield endoscopic techniques will aid in improving the sensitivity of detection of dysplasia and early cancer development in the esophagus.
Figures

References
-
- Williamson WA, Ellis FH, Jr, Gibb SP, Shahian DM, Aretz HT, Heatley GJ, Watkins E., Jr Barrett's esophagus. Prevalence and incidence of adenocarcinoma. Arch Intern Med. 1991;151:2212–6. - PubMed
-
- DeVault KR. Epidemiology and significance of Barrett's esophagus. Dig Dis. 2000;18:195–202. - PubMed
-
- Cameron AJ. Epidemiology of Barrett's esophagus and adenocarcinoma. Dis Esophagus. 2002;15:106–8. - PubMed
-
- Thomson BNJ, Cade RJ. Oesophagectomy for early adenocarcinoma and dysplasia arising in Barrett's oesophagus. Anz Journal of Surgery. 2003;73:121–124. - PubMed
-
- Dellon ES, Shaheen NJ. Does screening for Barrett's esophagus and adenocarcinorna of the esophagus prolong survival? Journal of Clinical Oncology. 2005;23:4478–4482. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
