

Repolarization and activation restitution near human pulmonary veins and atrial fibrillation initiation: a mechanism for the initiation of atrial fibrillation by premature beats
- PMID: 18926325
- PMCID: PMC2604131
- DOI: 10.1016/j.jacc.2008.07.012
Repolarization and activation restitution near human pulmonary veins and atrial fibrillation initiation: a mechanism for the initiation of atrial fibrillation by premature beats
Abstract
Objectives: The authors sought to study mechanisms to explain why single premature atrial complexes (PACs) from the pulmonary veins (PVs) may initiate human atrial fibrillation (AF).
Background: Theoretically, single PACs may initiate AF if the rate response of action potential duration (APD) restitution has a slope >1. However, human left atrial APD restitution and its relationship to AF have not been studied. We hypothesized that an APD restitution slope >1 near PVs explains the initiation of clinical AF.
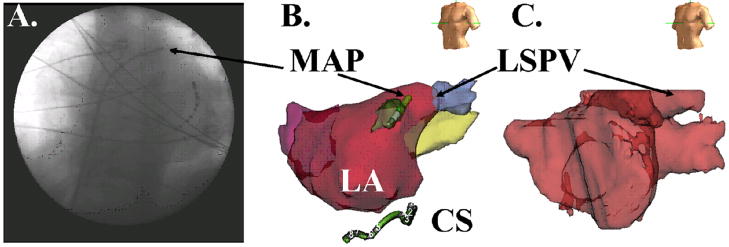
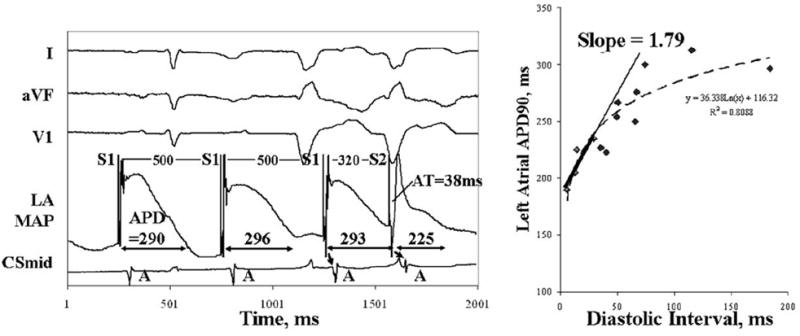
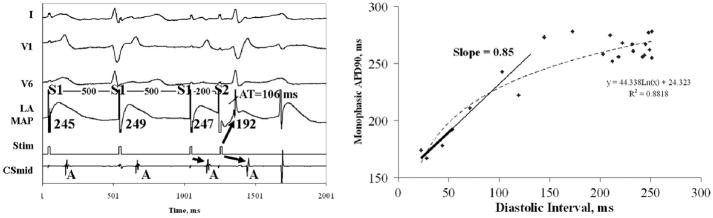
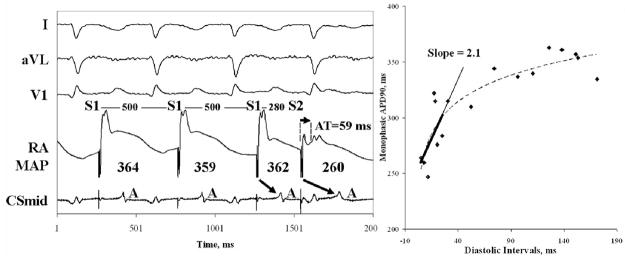
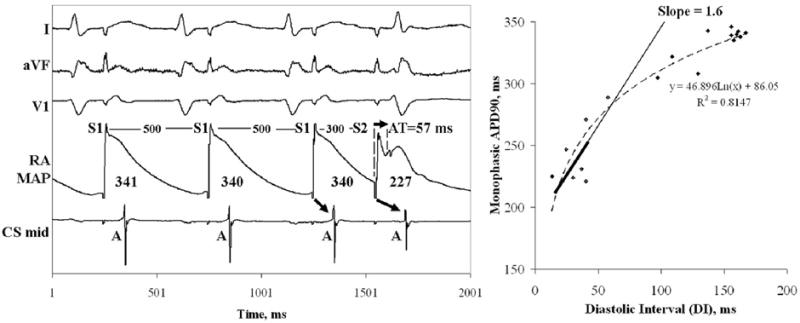
Methods: We studied 27 patients with paroxysmal and persistent (n = 13) AF. We advanced monophasic action potential catheters transseptally to superior PVs. Restitution was plotted as APD of progressively early PACs against their diastolic interval (DI) from prior beats. Activation time restitution was measured using the time from the pacing artifact to each PAC.
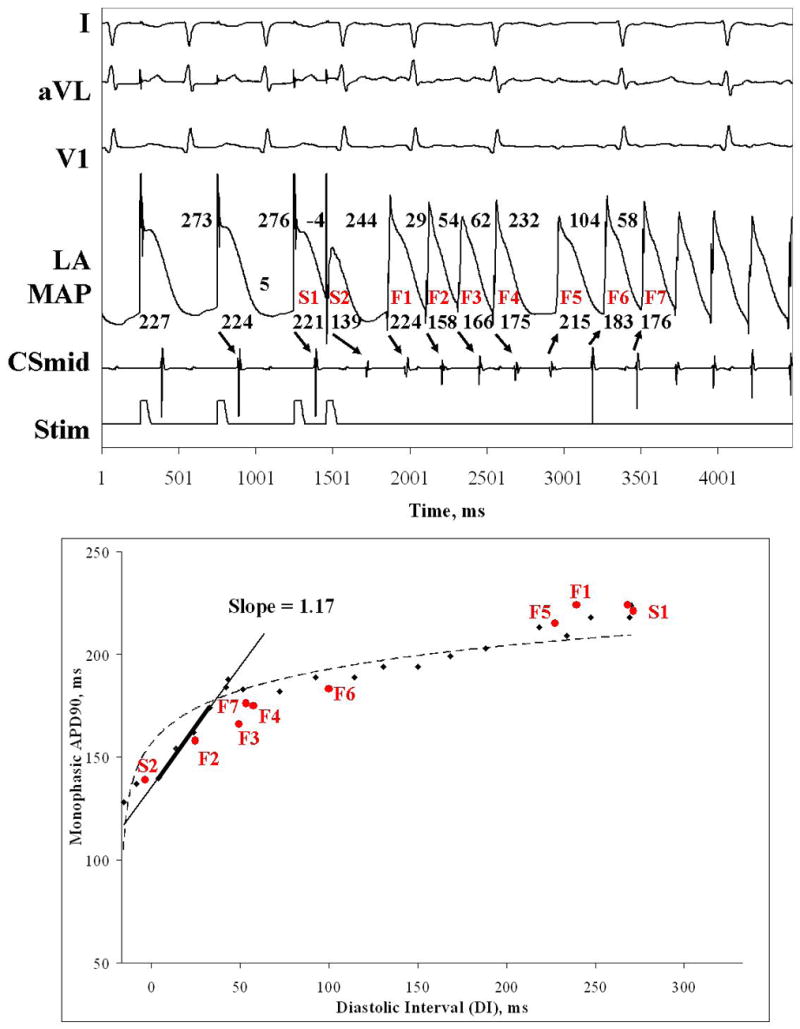
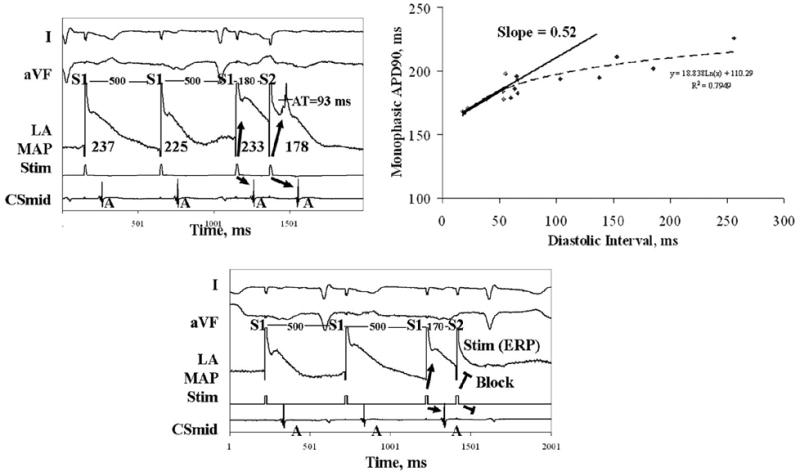
Results: Compared with paroxysmal AF, patients with persistent AF had shorter left atrial APD and effective refractory period (p = 0.01). In paroxysmal AF, maximum left atrial APD restitution slope was 1.5 +/- 0.4; and 12 of 13 patients had slope >1 (p < 0.001). In persistent AF, PACs encountered prolonged activation for a wider range of beats than in paroxysmal AF (p = 0.01), which prolonged DI and flattened APD restitution (slope 0.7 +/- 0.2; p < 0.001); no patient had APD restitution slope >1. A single PAC produced AF in 5 patients; in all, an APD restitution slope >1 caused extreme APD oscillations after the PAC, then AF.
Conclusions: In patients with paroxysmal AF, maximum APD restitution slope >1 near the PVs enables single PACs to initiate AF. However, patients with persistent AF show marked dynamic activation delay near PVs that flattens APD restitution. Studies should determine how regional APD and conduction dynamics contribute to the substrates of persistent AF.
Figures


References
-
- Haissaguerre M, Jais P, Shah DC, et al. Spontaneous Initiation of Atrial Fibrillation by Ectopic Beats Originating in the Pulmonary Veins. N Engl J Med. 1998;339:659–666. - PubMed
-
- Haissaguerre M, Sanders P, Hocini M, et al. Changes in Atrial Fibrillation Cycle Length and Inducibility During Catheter Ablation and Their Relation to Outcome. Circulation. 2004;109:3007–3013. - PubMed
-
- Gerstenfeld EP, Sauer W, Callans DJ, et al. Predictors of success after selective pulmonary vein isolation of arrhythmogenic pulmonary veins for treatment of atrial fibrillation. Heart Rhythm. 2006;3:165–170. - PubMed
-
- Haissaguerre M, Sanders P, Hocini M, et al. Catheter Ablation of Long-Lasting Persistent Atrial Fibrillation: Critical Structures for Termination. Journal of Cardiovascular Electrophysiology. 2005a;16:1125–1137. - PubMed
-
- Gong Y, Xie F, Stein K, et al. Mechanism underlying initiation of paroxysmal atrial flutter/atrial fibrillation by ectopic foci: a simulation study. Circulation. 2007;115:2094–102. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
