

Rapid reversal of human intestinal ischemia-reperfusion induced damage by shedding of injured enterocytes and reepithelialisation
- PMID: 18927609
- PMCID: PMC2561292
- DOI: 10.1371/journal.pone.0003428
Rapid reversal of human intestinal ischemia-reperfusion induced damage by shedding of injured enterocytes and reepithelialisation
Abstract
Background: Intestinal ischemia-reperfusion (IR) is a phenomenon related to physiological conditions (e.g. exercise, stress) and to pathophysiological events (e.g. acute mesenteric ischemia, aortic surgery). Although intestinal IR has been studied extensively in animals, results remain inconclusive and data on human intestinal IR are scarce. Therefore, an experimental harmless model for human intestinal IR was developed, enabling us to clarify the sequelae of human intestinal IR for the first time.
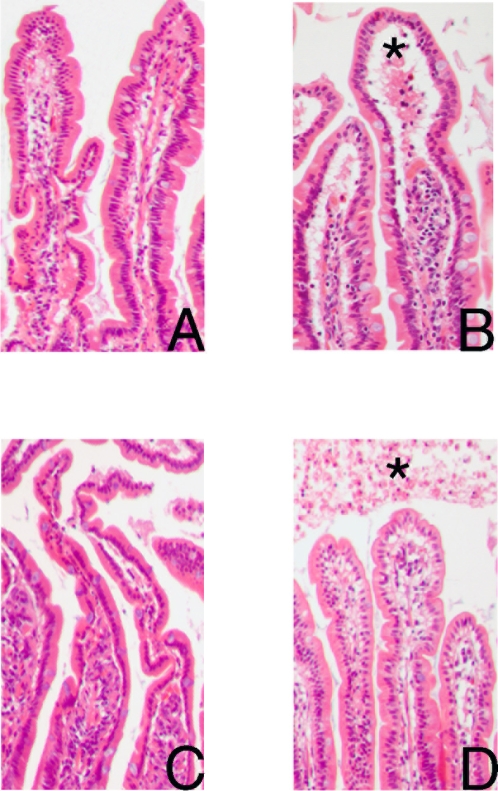
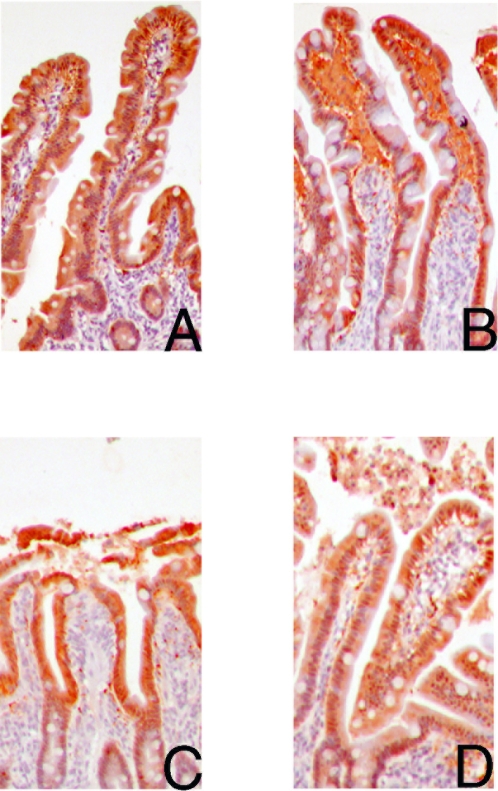
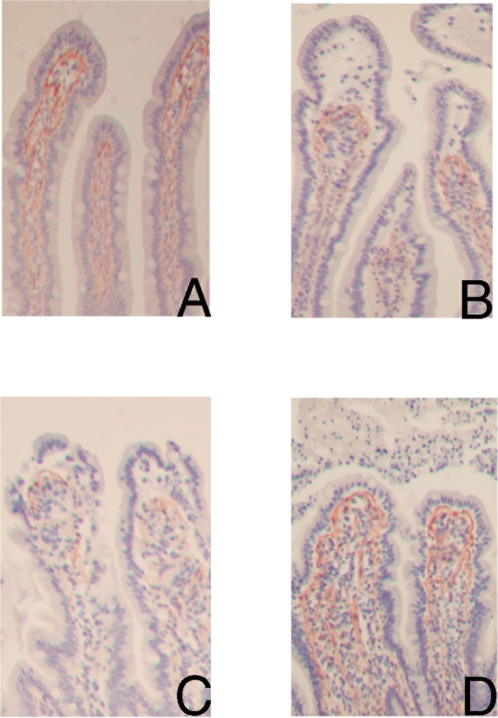
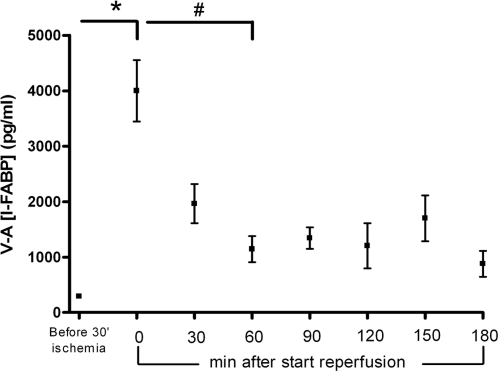
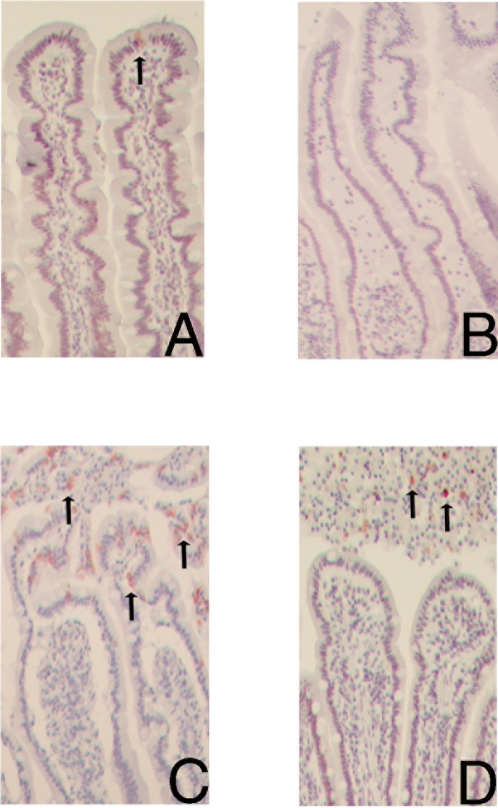
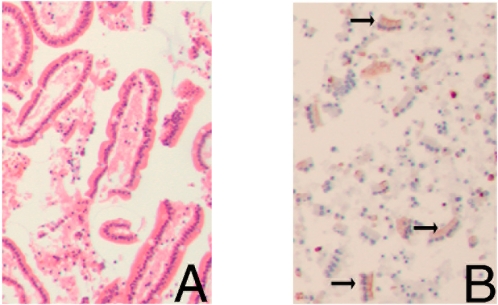
Methods and findings: In 30 patients undergoing pancreatico-duodenectomy we took advantage of the fact that in this procedure a variable length of jejunum is removed. Isolated jejunum (5 cm) was subjected to 30 minutes ischemia followed by reperfusion. Intestinal Fatty Acid Binding Protein (I-FABP) arteriovenous concentration differences across the bowel segment were measured before and after ischemia to assess epithelial cell damage. Tissue sections were collected after ischemia and at 25, 60 and 120 minutes reperfusion and stained with H&E, and for I-FABP and the apoptosis marker M30. Bonferroni's test was used to compare I-FABP differences. Mean (SEM) arteriovenous concentration gradients of I-FABP across the jejunum revealed rapidly developing epithelial cell damage. I-FABP release significantly increased from 290 (46) pg/ml before ischemia towards 3,997 (554) pg/ml immediately after ischemia (p<0.001) and declined gradually to 1,143 (237) pg/ml within 1 hour reperfusion (p<0.001). Directly after ischemia the intestinal epithelial lining was microscopically normal, while subepithelial spaces appeared at the villus tip. However, after 25 minutes reperfusion, enterocyte M30 immunostaining was observed at the villus tip accompanied by shedding of mature enterocytes into the lumen and loss of I-FABP staining. Interestingly, within 60 minutes reperfusion the epithelial barrier resealed, while debris of apoptotic, shedded epithelial cells was observed in the lumen. At the same time, M30 immunoreactivity was absent in intact epithelial lining.
Conclusions: This is the first human study to clarify intestinal IR induced cell damage and repair and its direct consequences. It reveals a unique, endogenous clearing mechanism for injured enterocytes: rapid detachment of damaged apoptotic enterocytes into the lumen. This process is followed by repair of the epithelial continuity within an hour, resulting in a normal epithelial lining.
Conflict of interest statement
Figures
References
-
- American Gastroenterological Association Medical Position Statement: guidelines on intestinal ischemia. Gastroenterology. 2000;118:951–953. - PubMed
-
- Oldenburg WA, Lau LL, Rodenberg TJ, Edmonds HJ, Burger CD. Acute mesenteric ischemia: a clinical review. Arch Intern Med. 2004;164:1054–1062. - PubMed
-
- Jeukendrup AE, Vet-Joop K, Sturk A, Stegen JHJC, Senden J, et al. Relationship between gastro-intestinal complaints and endotoxaemia, cytokine release and the acute-phase reaction during and after a long-distance triathlon in highly trained men. Clin Science. 2000;98:47–55. - PubMed
-
- Rokyta R, Matejovic M, Novak I, Zeman V, Krouzecky A, et al. Submaximal exercise in healthy volunteers: the relationship between gastric mucosal and systemic energy status. Pflügers Arch - Eur J Physiol. 2002;443:852–857. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
