

Complement activation fragment Bb in early pregnancy and spontaneous preterm birth
- PMID: 18928972
- PMCID: PMC2586079
- DOI: 10.1016/j.ajog.2008.07.044
Complement activation fragment Bb in early pregnancy and spontaneous preterm birth
Abstract
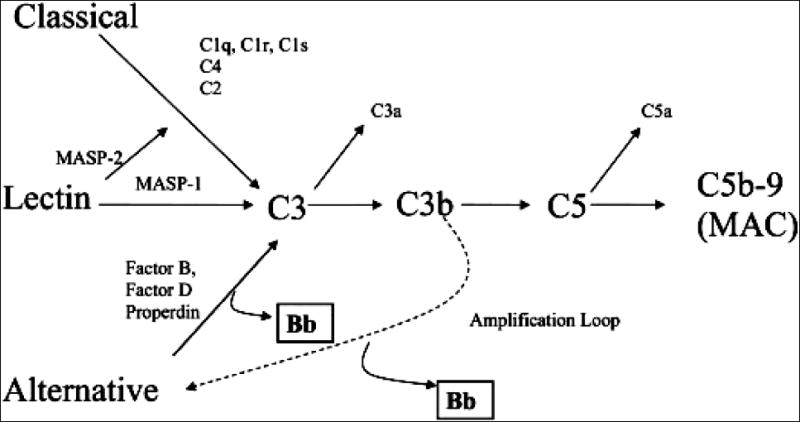
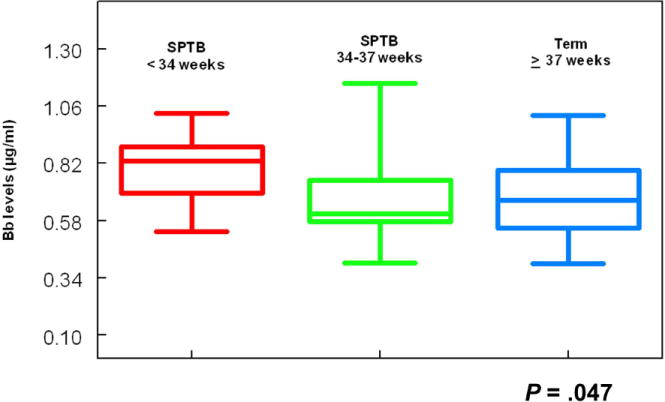
Objective: The objective of this study was to determine whether an elevated level of the complement activation fragment Bb in early pregnancy was associated with spontaneous preterm birth (SPTB) at less than 34 weeks' gestation or SPTB between 34 and 37 weeks' gestation (late SPTB).
Study design: This was a prospective study of 784 women enrolled at less than 20 weeks' gestation.
Results: Following exclusions, 13 women (1.7%) had a SPTB at less than 34 weeks' gestation and 25 (3.2%) a SPTB between 34 and 37 weeks' gestation. Women with Bb in the top quartile were 4.7 times more likely to have an SPTB less than 34 weeks' gestation as compared with women who had levels of Bb in the lower 3 quartiles (95% confidence interval [CI] 1.5-14, P = .003). There was no association between Bb and late SPTB (relative risk 0.8, 95% CI 0.3-2).
Conclusion: A significant relationship was found between an elevated Bb in early pregnancy and SPTB less than 34 weeks' gestation. These results suggest that inflammatory events in early pregnancy are part of the pathogenic mechanisms of this condition.
Figures
Comment in
-
Immune activation early in pregnancy: trouble down the road?Am J Obstet Gynecol. 2008 Oct;199(4):327-8. doi: 10.1016/j.ajog.2008.06.053. Am J Obstet Gynecol. 2008. PMID: 18928970 No abstract available.
Similar articles
-
Fragment Bb in amniotic fluid: evidence for complement activation by the alternative pathway in women with intra-amniotic infection/inflammation.J Matern Fetal Neonatal Med. 2009 Oct;22(10):905-16. doi: 10.1080/14767050902994663. J Matern Fetal Neonatal Med. 2009. PMID: 19603351 Free PMC article.
-
Cervical elastography in predicting spontaneous preterm birth in singleton pregnancy with a short cervix receiving progesterone treatment at 18 to 24 weeks' gestation.J Matern Fetal Neonatal Med. 2024 Dec;37(1):2347954. doi: 10.1080/14767058.2024.2347954. Epub 2024 May 7. J Matern Fetal Neonatal Med. 2024. PMID: 38714523
-
Alternative complement pathway activation fragment Bb in early pregnancy as a predictor of preeclampsia.Am J Obstet Gynecol. 2008 Apr;198(4):385.e1-9. doi: 10.1016/j.ajog.2007.10.793. Epub 2008 Jan 25. Am J Obstet Gynecol. 2008. PMID: 18221926 Free PMC article.
-
Efficacy of transvaginal cervical cerclage in women at risk of preterm birth following previous emergency cesarean section.Acta Obstet Gynecol Scand. 2020 Nov;99(11):1486-1491. doi: 10.1111/aogs.13972. Epub 2020 Sep 2. Acta Obstet Gynecol Scand. 2020. PMID: 32777082
-
Risk of spontaneous preterm birth in singleton pregnancies conceived after IVF/ICSI treatment: meta-analysis of cohort studies.Ultrasound Obstet Gynecol. 2018 Jan;51(1):43-53. doi: 10.1002/uog.18930. Ultrasound Obstet Gynecol. 2018. PMID: 29114987 Review.
Cited by
-
Alternative pathway activation in pregnancy, a measured amount "complements" a successful pregnancy, too much results in adverse events.Immunol Rev. 2023 Jan;313(1):298-319. doi: 10.1111/imr.13169. Epub 2022 Nov 15. Immunol Rev. 2023. PMID: 36377667 Free PMC article. Review.
-
Elevated Adipsin and Reduced C5a Levels in the Maternal Serum and Follicular Fluid During Implantation Are Associated With Successful Pregnancy in Obese Women.Front Endocrinol (Lausanne). 2022 Jul 13;13:918320. doi: 10.3389/fendo.2022.918320. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35909516 Free PMC article.
-
The Microbiome and Complement Activation: A Mechanistic Model for Preterm Birth.Biol Res Nurs. 2017 May;19(3):295-307. doi: 10.1177/1099800416687648. Epub 2017 Jan 11. Biol Res Nurs. 2017. PMID: 28073296 Free PMC article. Review.
-
Complement activation, a threat to pregnancy.Semin Immunopathol. 2018 Jan;40(1):103-111. doi: 10.1007/s00281-017-0645-x. Epub 2017 Sep 12. Semin Immunopathol. 2018. PMID: 28900713 Review.
-
Low Levels of Complement Factor H in the First Trimester of Pregnancy Are Associated with Spontaneous Preterm Birth.Int J Mol Sci. 2024 Sep 30;25(19):10549. doi: 10.3390/ijms251910549. Int J Mol Sci. 2024. PMID: 39408876 Free PMC article.
References
-
- Gibbs RS. The relationship between infections and adverse pregnancy outcomes: an overview. Ann Periodontol. 2001;6(1):153–63. - PubMed
-
- Goldenberg RL, Hauth JC, Andrews WW. Intrauterine infection and preterm delivery. N Engl J Med. 2000;342(20):1500–7. - PubMed
-
- Buekens P, Klebanoff M. Preterm birth research: from disillusion to the search for new mechanisms. Paediatr Perinat Epidemiol. 2001;15 Suppl 2:159–61. - PubMed
-
- Green NS, Damus K, Simpson JL, Iams J, Reece EA, Hobel CJ, et al. Research agenda for preterm birth: recommendations from the March of Dimes. Am J Obstet Gynecol. 2005;193(3 Pt 1):626–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
