

k-Space and time sensitivity encoding-accelerated myocardial perfusion MR imaging at 3.0 T: comparison with 1.5 T
- PMID: 18936311
- PMCID: PMC2586821
- DOI: 10.1148/radiol.2492080017
k-Space and time sensitivity encoding-accelerated myocardial perfusion MR imaging at 3.0 T: comparison with 1.5 T
Abstract
Purpose: To determine the feasibility and diagnostic accuracy of high-spatial-resolution myocardial perfusion magnetic resonance (MR) imaging at 3.0 T by using k-space and time (k-t) domain undersampling with sensitivity encoding (SENSE), or k-t SENSE. Data were compared with results of k-t SENSE-accelerated high-spatial-resolution perfusion MR imaging at 1.5 T and standard-resolution acquisition at 3.0 T.
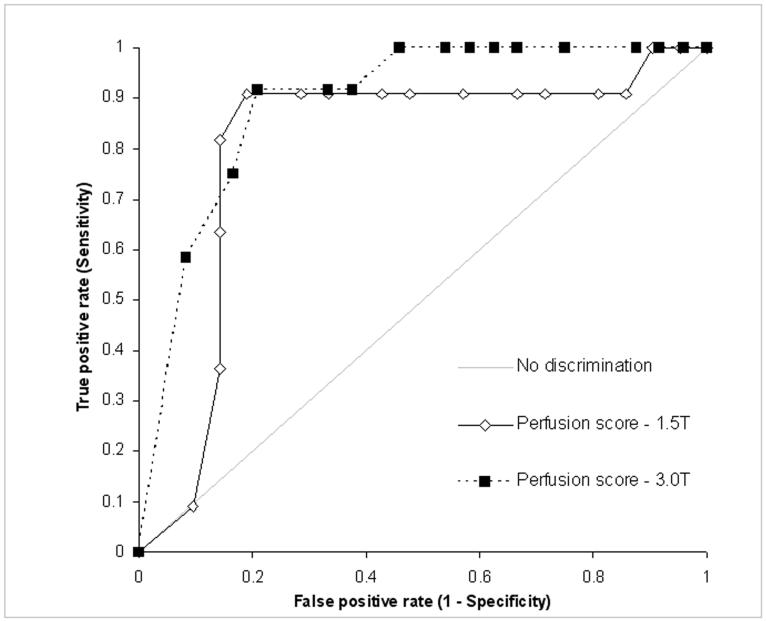
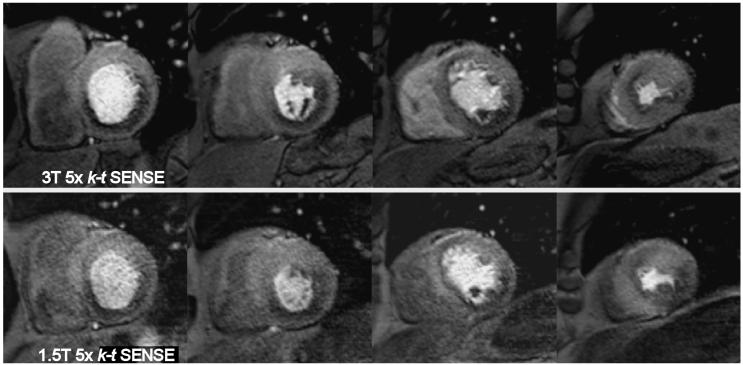
Materials and methods: The study was reviewed and approved by the local ethics review board; informed consent was obtained. k-t SENSE perfusion MR imaging was performed at 1.5 and 3.0 T (fivefold k-t SENSE acceleration; spatial resolution, 1.3 x 1.3 x 10 mm). Fourteen volunteers were studied at rest; 37 patients were studied during adenosine-induced stress. In volunteers, comparison was also made with standard-resolution (2.5 x 2.5 x 10 mm) twofold SENSE perfusion MR imaging results at 3.0 T. Image quality, artifact scores, signal-to-noise ratios (SNRs), and contrast enhancement ratios were derived. In patients, diagnostic accuracy of visual analysis to detect stenosis of more than 50% narrowing in diameter at quantitative coronary angiography was determined by using receiver operator characteristic (ROC) analysis.
Results: In volunteers, image quality and artifact scores were similar for 3.0- and 1.5-T k-t SENSE perfusion MR imaging, while SNR was higher (11.6 vs 5.6) and contrast enhancement ratio was lower (1.1 vs 1.5, P = .012) at 3.0 T. Compared with standard-resolution perfusion MR imaging, image quality was higher for 3.0-T k-t SENSE (3.6 vs 3.1, P = .04), endocardial dark rim artifacts were reduced (artifact thickness, 1.6 vs 2.4 mm, P < .001), and contrast enhancement ratios were similar. In patients, areas under the ROC curve for detection of coronary stenosis were 0.89 and 0.80 (P = .21) for 3.0 and 1.5 T, respectively.
Conclusion: k-t SENSE-accelerated high-spatial-resolution perfusion MR imaging at 3.0 T is feasible, with similar artifacts and diagnostic accuracy as those at 1.5 T. Compared with standard-resolution twofold SENSE perfusion MR imaging, image quality at k-t SENSE MR imaging is improved and artifacts are reduced.
(c) RSNA, 2008.
Figures





References
-
- Cheng AS, Pegg TJ, Karamitsos TD, Searle N, Jerosch-Herold M, Choudhury RP, Banning AP, Neubauer S, Robson MD, Selvanayagam JB. Cardiovascular magnetic resonance perfusion imaging at 3-tesla for the detection of coronary artery disease: a comparison with 1.5-tesla. J Am Coll Cardiol. 2007;49:2440–9. - PubMed
-
- Araoz PA, Glockner JF, McGee KP, et al. 3 Tesla MR imaging provides improved contrast in first-pass myocardial perfusion imaging over a range of gadolinium doses. J Cardiovasc Magn Reson. 2005;7:559–64. - PubMed
-
- Gutberlet M, Noeske R, Schwinge K, et al. Comprehensive cardiac magnetic resonance imaging at 3.0 Tesla: feasibility and implications for clinical applications. Invest Radiol. 2006;41:154–67. - PubMed
-
- Gutberlet M, Spors B, Grothoff M, et al. Comparison of different cardiac MRI sequences at 1.5 T/3.0 T with respect to signal-to-noise and contrast-to-noise ratios—initial experience. Rofo. 2004;176:801–8. - PubMed
-
- Theisen D, Wintersperger BJ, Huber A, Dietrich O, Reiser MF, Schonberg SO. Myocardial perfusion imaging with Gadobutrol: a comparison between 3 and 1.5 Tesla with an identical sequence design. Invest Radiol. 2007;42:499–506. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
