

Patients with acute stroke treated with intravenous tPA 3-6 hours after stroke onset: correlations between MR angiography findings and perfusion- and diffusion-weighted imaging in the DEFUSE study
- PMID: 18936316
- PMCID: PMC2657860
- DOI: 10.1148/radiol.2492071751
Patients with acute stroke treated with intravenous tPA 3-6 hours after stroke onset: correlations between MR angiography findings and perfusion- and diffusion-weighted imaging in the DEFUSE study
Abstract
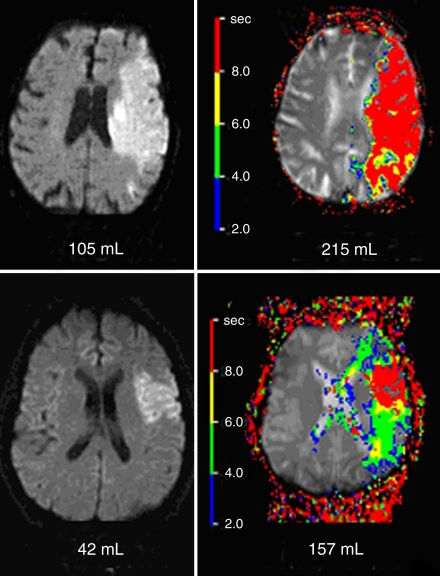
Purpose: To study magnetic resonance (MR) angiography findings in patients with acute stroke treated with intravenous tissue plasminogen activator (tPA) in relationship to perfusion- and diffusion-weighted imaging changes and clinical outcome.
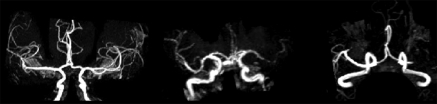
Materials and methods: Patients treated with intravenous tPA 3-6 hours after stroke onset (with informed consent) were evaluated in a HIPAA-compliant multicenter prospective study approved by all institutional review boards. MR imaging and MR angiography studies were performed before and 3-6 hours after treatment. MR angiography studies that were technically adequate at both time points were evaluated for occlusion, decreased flow, any early recanalization, and degree of recanalization. These results were compared with favorable clinical response (an improvement in National Institutes of Health Stroke Scale score of >or=8 points at 30 days or a modified Rankin scale score of 0 or 1 at 30 days) in patients with and those without mismatch between perfusion- and diffusion-weighted imaging at baseline.
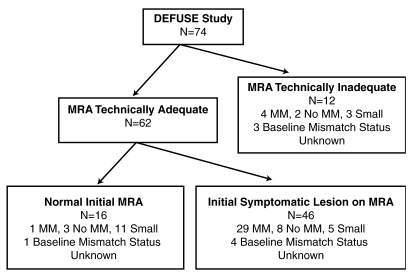
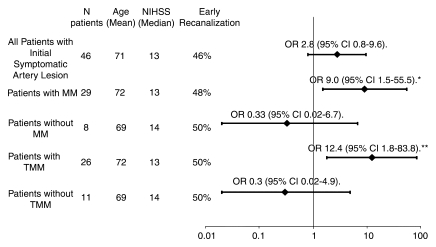
Results: Seventy-four patients were enrolled in the initial investigation; pre- and posttreatment MR angiography studies were both technically adequate in 62 patients. MR angiography demonstrated occlusion or decreased flow in 46 patients. Patients with isolated middle cerebral artery (MCA) occlusion and early recanalization at MR angiography had higher rates of favorable clinical response than those with tandem internal carotid artery-MCA occlusion and early recanalization (P = .05). Any early recanalization was not associated with favorable clinical response, but degree of recanalization did correlate with favorable clinical response (P = .048). Favorable clinical response was more frequently seen in patients with mismatch between perfusion- and diffusion-weighted imaging findings at baseline who experienced early recanalization than in those who did not have early recanalization (odds ratio = 6.2; 95% confidence interval: 1.3, 30.2; P = .021). No relationship between early recanalization and favorable clinical response was seen in patients without mismatch.
Conclusion: Early recanalization seen at MR angiography before and after treatment coupled with diffusion- and perfusion-weighted imaging data may predict clinical outcome in patients with stroke treated with tPA 3-6 hours after symptom onset.
(c) RSNA, 2008.
Figures
References
-
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med 1995;333:1581–1587. - PubMed
-
- Clark WM, Wissman S, Albers GW, Jhamandas JH, Madden KP, Hamilton S. Recombinant tissue-type plasminogen activator (Alteplase) for ischemic stroke 3 to 5 hours after symptom onset: the ATLANTIS study—a randomized controlled trial. Alteplase thrombolysis for acute noninterventional therapy in ischemic stroke. JAMA 1999;282:2019–2026. - PubMed
-
- Hacke W, Kaste M, Fieschi C, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA 1995;274:1017–1025. - PubMed
-
- Hacke W, Kaste M, Fieschi C, et al. Randomized double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischemic stroke. (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet 1998;352:1245–1251. - PubMed
-
- Parsons MW, Barber PA, Chalk J, et al. Diffusion- and perfusion-weighted MRI response to thrombolysis in stroke. Ann Neurol 2002;51:28–37. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
