

Factors associated with the use of evidence-based therapies after discharge among elderly patients with myocardial infarction
- PMID: 18936455
- PMCID: PMC2565714
- DOI: 10.1503/cmaj.080295
Factors associated with the use of evidence-based therapies after discharge among elderly patients with myocardial infarction
Abstract
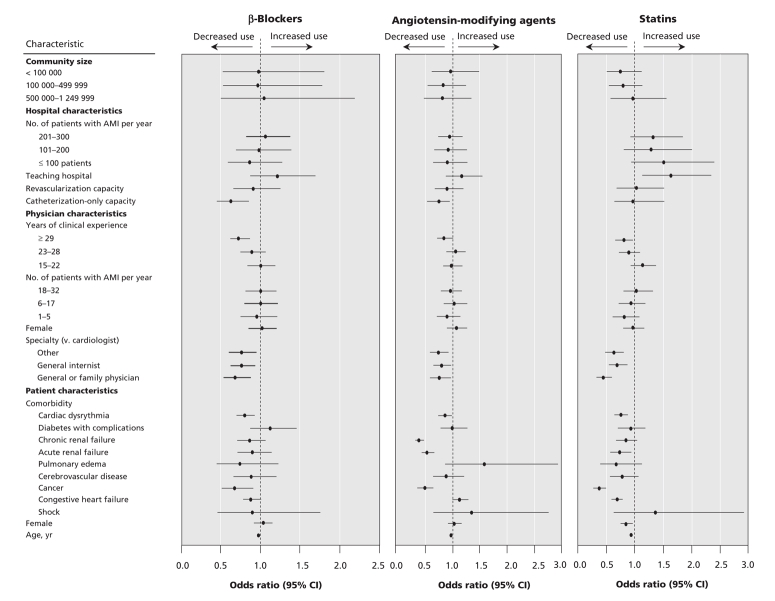
Background: In an accompanying article, we report moderate between-hospital variation in the postdischarge use of beta-blockers, angiotensin-modifying drugs and statins by elderly patients who had been admitted to hospital with acute myocardial infarction. Our objective was to identify the characteristics of patients, physicians, hospitals and communities associated with differences in the use of these medications after discharge.
Methods: For this retrospective, population-based cohort study, we used linked administrative databases. We examined data for all patients aged 65 years or older who were discharged from hospital in 2005/06 with a diagnosis of myocardial infarction. We determined the effect of patient, physician, hospital and community characteristics on the rate of postdischarge medication use.
Results: Increasing patient age was associated with lower postdischarge use of medications. The odds ratios (ORs) for a 1-year increase in age were 0.98 (95% confidence interval [CI] 0.97-0.99) for beta-blockers, 0.97 (95% CI 0.97-0.98) for angiotensin-converting-enzyme inhibitors and angiotensin-receptor blockers and 0.94 (95% CI 0.93-0.95) for statins. Having a general or family practitioner, a general internist or a physician of another specialty as the attending physician, relative to having a cardiologist, was associated with lower postdischarge use of beta-blockers, angiotensin-modifying agents and statins (ORs ranging from 0.46 to 0.82). Having an attending physician with 29 or more years experience, relative to having a physician who had graduated within the past 15 years, was associated with lower use of beta-blockers (OR 0.71, 95% CI 0.60-0.84) and statins (OR 0.81, 95% CI 0.67-0.97).
Interpretation: Patients who received care from noncardiologists and physicians with at least 29 years of experience had substantially lower use of evidence-based drug therapies after discharge. Dissemination strategies should be devised to improve the prescribing of evidence-based medications by these physicians.
Figures
Comment in
-
Myocardial infarction and quality of care.CMAJ. 2008 Oct 21;179(9):875-6. doi: 10.1503/cmaj.081438. CMAJ. 2008. PMID: 18936445 Free PMC article. Review. No abstract available.
References
-
- Soumerai SB, McLaughlin TJ, Spiegelman D, et al. Adverse outcomes of underuse of β-blockers in elderly survivors of acute myocardial infarction. JAMA 1997;277:115-21. - PubMed
-
- Gurwitz JH, Goldberg RJ, Chen Z, et al. β-Blocker therapy in acute myocardial infarction: evidence for underutilization in the elderly. Am J Med 1992;93:605-10. - PubMed
-
- Barron HV, Michaels AD, Maynard C, et al. Use of antiotensin-converting enzyme inhibitors at discharge in patients with acute myocardial infarction in the United States: data from the National Registry of Myocardial Infarction 2. J Am Coll Cardiol 1998;32:360-7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous