

Indicators of quality of care for patients with acute myocardial infarction
- PMID: 18936456
- PMCID: PMC2565729
- DOI: 10.1503/cmaj.080749
Indicators of quality of care for patients with acute myocardial infarction
Abstract
Background: There is a wide practice gap between optimal and actual care for patients with acute myocardial infarction in hospitals around the world. We undertook this initiative to develop an updated set of evidence-based indicators to measure and improve the quality of care for this patient population.
Methods: A 12-member expert panel was convened in 2007 to develop an updated set of quality indicators for acute myocardial infarction. The panel identified a list of potential indicators after reviewing the scientific literature, clinical practice guidelines and other published quality indicators. To develop the new list of indicators, the panel rated each potential indicator on 4 dimensions (reliability, validity, feasibility and usefulness in improving patient outcomes) and discussed the top-ranked quality indicators at a consensus meeting.
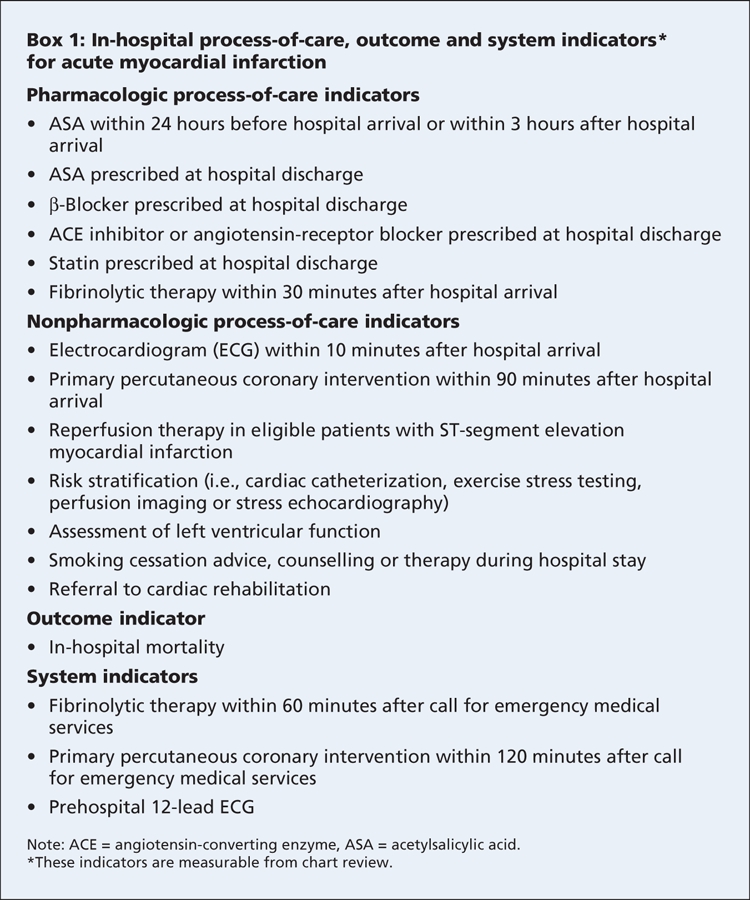
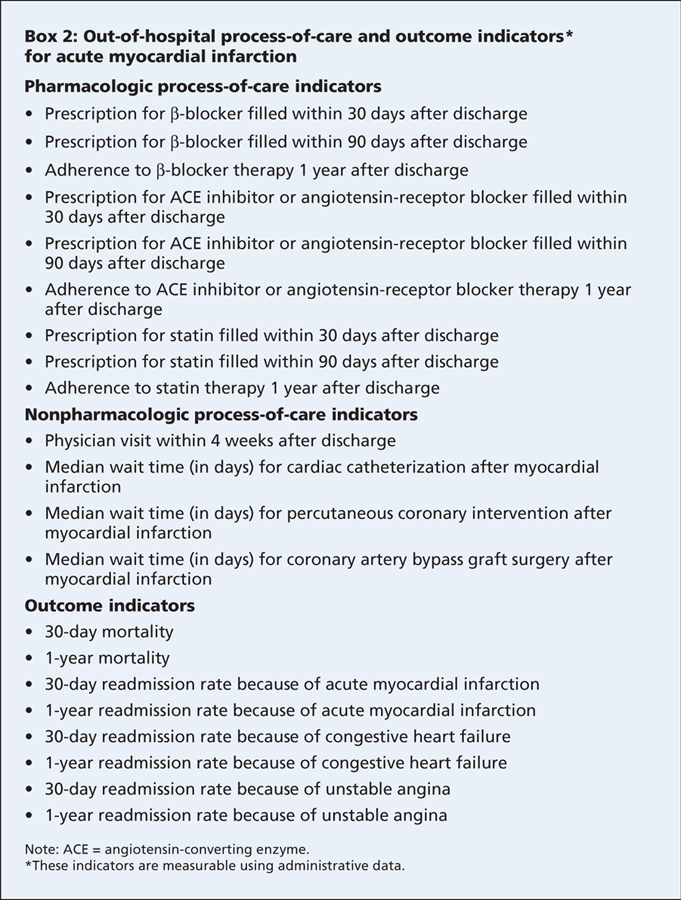
Results: Consensus was reached on 38 quality indicators: 17 that would be measurable using chart-abstracted data and 21 that would be measurable using administrative data. Of the 17 chart-review indicators, 13 address pharmacologic and nonpharmacologic care delivered to patients in hospital. In-hospital mortality was recommended as a key outcome indicator. Three system indicators were recommended to measure the collaborative responsiveness of the health care system from the call for help to intervention. It was recommended that hospitals strive for a minimum target benchmark of 90% or greater on process-of-care indicators.
Interpretation: Implementation of strategies by clinicians and hospitals to meet target benchmarks on these quality indicators could save the lives of many individuals with acute myocardial infarction.
References
-
- Fox KA, Goodman SG, Klein W, et al. Management of acute coronary syndromes. Variations in practice and outcome: findings from the Global Registry of Acute Coronary Events (GRACE). Eur Heart J 2002;23:1177-89. - PubMed
-
- Fox KA, Steg PG, Eagle KA, et al. Decline in rates of death and heart failure in acute coronary syndromes, 1999–2006. JAMA 2007;297:1892-900. - PubMed
-
- Eagle KA, Nallamothu BK, Mehta RH, et al. Trends in acute reperfusion therapy for ST-segment elevation myocardial infarction from 1999 to 2006: We are getting better but we have got a long way to go. Eur Heart J 2008;29:609-17. - PubMed
-
- Lenfant C. Shattuck lecture. Clinical research to clinical practice: Lost in translation? N Engl J Med 2003;349:868-74. - PubMed
-
- Spertus JA, Eagle KA, Krumholz HM, et al. American College of Cardiology and American Heart Association methodology for the selection and creation of performance measures for quantifying the quality of cardiovascular care. Circulation 2005;111:1703-12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous