

Cost-effectiveness of nurse-led disease management for heart failure in an ethnically diverse urban community
- PMID: 18936502
- PMCID: PMC4312002
- DOI: 10.7326/0003-4819-149-8-200810210-00006
Cost-effectiveness of nurse-led disease management for heart failure in an ethnically diverse urban community
Abstract
Background: Randomized, controlled trials have shown that nurse-led disease management for patients with heart failure can reduce hospitalizations. Less is known about the cost-effectiveness of these interventions.
Objective: To estimate the cost-effectiveness of a nurse-led disease management intervention over 12 months, implemented in a randomized, controlled effectiveness trial.
Design: Cost-effectiveness analysis conducted alongside a randomized trial.
Data sources: Medical costs from administrative records, and self-reported quality of life and nonmedical costs from patient surveys.
Participants: Patients with systolic dysfunction recruited from ambulatory clinics in Harlem, New York.
Time horizon: 12 months.
Perspective: Societal and payer.
Intervention: 12-month program that involved 1 face-to-face encounter with a nurse and regular telephone follow-up.
Outcome measures: Quality of life as measured by the Health Utilities Index Mark 3 and EuroQol-5D and cost-effectiveness as measured by the incremental cost-effectiveness ratio (ICER).
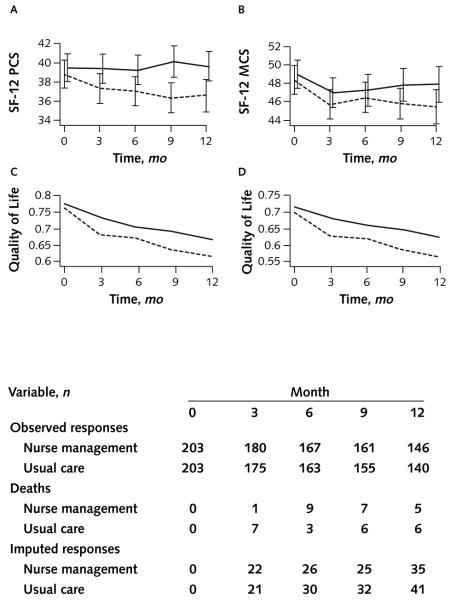
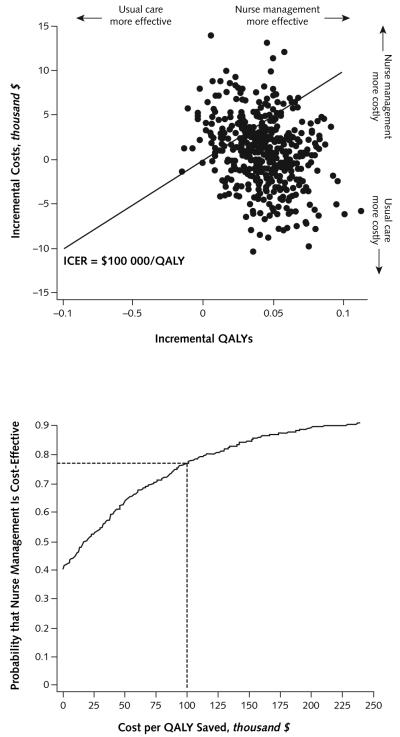
Results of base-case analysis: Costs and quality of life were higher in the nurse-managed group than the usual care group. The ICERs over 12 months were $17,543 per EuroQol-5D-based quality-adjusted life-year (QALY) and $15,169 per Health Utilities Index Mark 3-based QALY (in 2001 U.S. dollars).
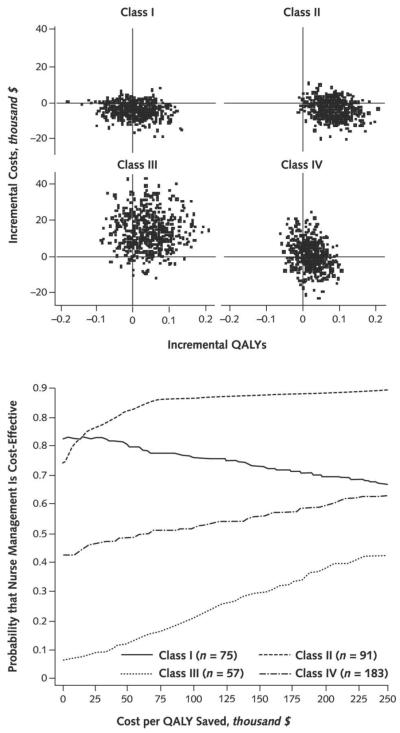
Results of sensitivity analysis: From a payer perspective, the ICER ranged from $3673 to $4495 per QALY. Applying national prices in place of New York City prices yielded a societal ICER of $13,460 to $15,556 per QALY. Cost-effectiveness acceptability curves suggest that the intervention was most likely cost-effective for patients with less severe (New York Heart Association classes I to II) heart failure.
Limitation: The trial was conducted in an ethnically diverse, inner-city neighborhood; thus, results may not be generalizable to other communities.
Conclusion: Over 12 months, the nurse-led disease management program was a reasonably cost-effective way to reduce the burden of heart failure in this community.
Figures
Comment in
-
Nurse-led heart failure management improved quality of life and was cost-effective.Evid Based Nurs. 2009 Apr;12(2):59. doi: 10.1136/ebn.12.2.59. Evid Based Nurs. 2009. PMID: 19321836 No abstract available.
References
-
- McAlister FA, Lawson FM, Teo KK, Armstrong PW. A systematic review of randomized trials of disease management programs in heart failure. Am J Med. 2001;110:378–84. [PMID: 11286953] - PubMed
-
- Gold M, Siegel J, Russell L, Weinstein M. Cost-Effectiveness in Health and Medicine. Oxford Univ Pr; New York: 1996.
-
- Rosamond W, Flegal K, Friday G, Furie K, Go A, Greenlund K, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69–171. [PMID: 17194875] - PubMed
-
- Ghali JK, Kadakia S, Cooper R, Ferlinz J. Precipitating factors leading to decompensation of heart failure. Traits among urban blacks. Arch Intern Med. 1988;148:2013–6. [PMID: 3046541] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials