

Case Reports
. 2008 Oct;22(10):2385-8; discussion 2388.
doi: 10.1089/end.2008.0338.
Pediatric robot-assisted laparoscopic excision of urachal cyst and bladder cuff
Affiliations
- PMID: 18937602
- PMCID: PMC3141736
- DOI: 10.1089/end.2008.0338
Item in Clipboard
Case Reports
Pediatric robot-assisted laparoscopic excision of urachal cyst and bladder cuff
J Endourol.
2008 Oct.
Abstract
Urachal cysts are the most common urachal anomaly in the pediatric population. There is an increasing body of literature documenting successful management of urachal cysts using laparoscopic techniques. There may be an advantage, however, with the use of robot-assisted laparoscopy for reconstructive cases. We describe the techniques used for robot-assisted laparoscopic excision of a urachal cyst and bladder cuff with bladder repair in a female child. This approach is a safe and effective option for the minimally invasive management of pediatric urachal cysts.
Figures
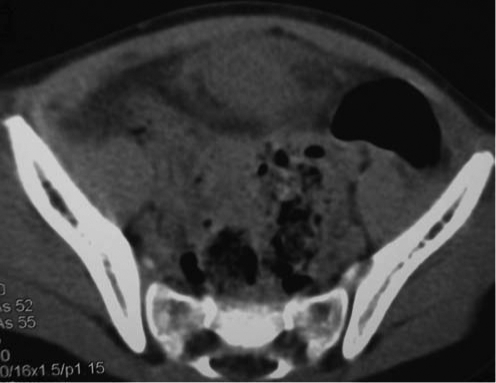
A CT scan of the abdomen shows a midline anterior cystic mass just superior to the bladder with local inflammation consistent with an inflamed urachal cyst.
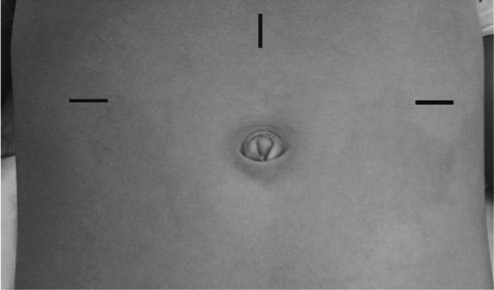
A 12-mm camera port is placed through a vertical incision at midline halfway between the umbilicus and the xyphoid process; 5- or 8-mm ports are placed through horizontal incisions at the anterior axillary lines just superior to level of umbilicus
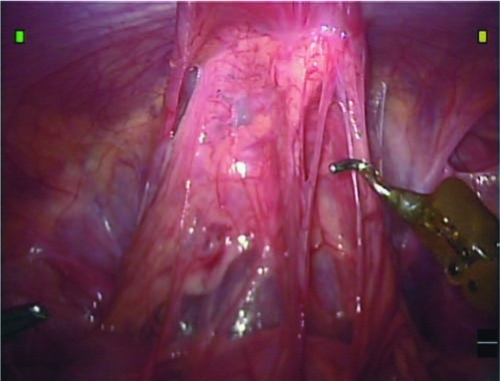
Omental adhesions cover the urachal cyst.
Dissection of the urachus from the anterior abdominal wall occurs after division of the right obliterated umbilical artery.
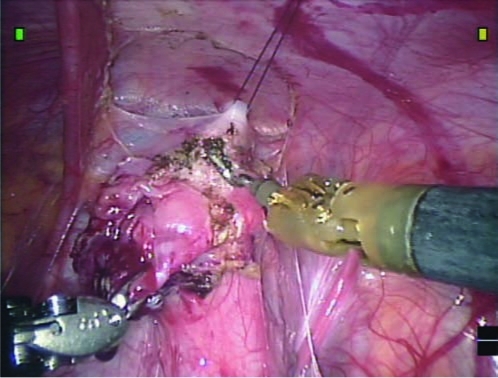
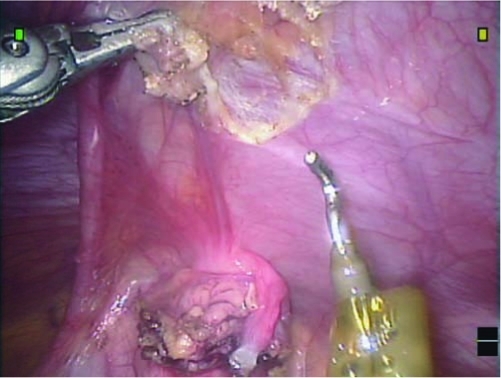
With the hitch stitch providing countertraction, the urachal cyst and bladder cuff are excised from the rest of the bladder.
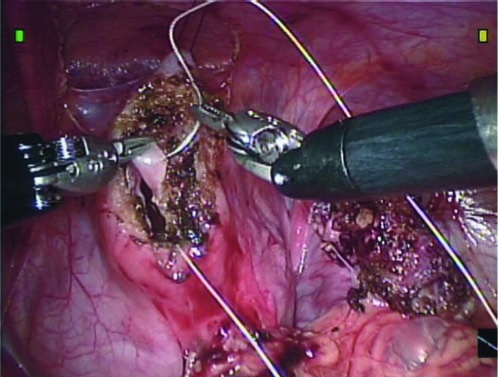
Two layer closure of the bladder opening is used after excision of the urachal cyst and bladder cuff.
References
-
- Ashley RA. Inman BA. Routh JC. Rohlinger RA. Husmann DA. Kramer SA. Urachal anomalies: A longitudinal study of urachal remnants in children and adults. J Urol. 2007;178:1615–1618. - PubMed
-
- McCollum MO. Macneily AE. Blair GK. Surgical implications of urachal remnants: Presentation and management. J Pediatr Surg. 2003;38:798–803. - PubMed
-
- Bauer SB. Retik AB. Urachal anomalies and related umbilical disorders. Urol Clin North Am. 1978;5:195–211. - PubMed
-
- Cilento BG., Jr Bauer SB. Retik AB. Peters CA. Atala A. Urachal anomalies: Defining the best diagnostic modality. Urology. 1998;52:120–122. - PubMed
-
- Madeb R. Knopf JK. Nicholson C, et al. The use of robotically assisted surgery for treating urachal anomalies. BJU Int. 2006;98:838–842. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
