

Perioperative oxygen fraction - effect on surgical site infection and pulmonary complications after abdominal surgery: a randomized clinical trial. Rationale and design of the PROXI-Trial
- PMID: 18945347
- PMCID: PMC2600782
- DOI: 10.1186/1745-6215-9-58
Perioperative oxygen fraction - effect on surgical site infection and pulmonary complications after abdominal surgery: a randomized clinical trial. Rationale and design of the PROXI-Trial
Abstract
Background: A high perioperative inspiratory oxygen fraction may reduce the risk of surgical site infections, as bacterial eradication by neutrophils depends on wound oxygen tension. Two trials have shown that a high perioperative inspiratory oxygen fraction (FiO(2) = 0.80) significantly reduced risk of surgical site infections after elective colorectal surgery, but a third trial was stopped early because the frequency of surgical site infections was more than doubled in the group receiving FiO(2) = 0.80. It has not been settled if a high inspiratory oxygen fraction increases the risk of pulmonary complications, such as atelectasis, pneumonia and respiratory failure. The aim of our trial is to assess the potential benefits and harms of a high perioperative oxygen fraction in patients undergoing abdominal surgery.
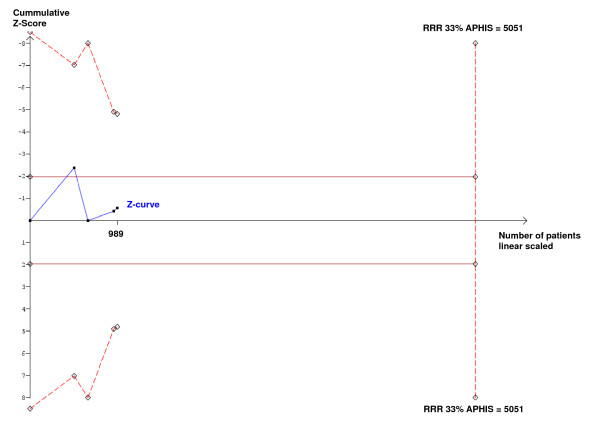
Methods and design: The PROXI-Trial is a randomized, patient- and assessor blinded trial of perioperative supplemental oxygen in 1400 patients undergoing acute or elective laparotomy in 14 Danish hospitals. Patients are randomized to receive either 80% oxygen (FiO(2) = 0.80) or 30% oxygen (FiO(2) = 0.30) during surgery and for the first 2 postoperative hours. The primary outcome is surgical site infection within 14 days. The secondary outcomes are: atelectasis, pneumonia, respiratory failure, re-operation, mortality, duration of postoperative hospitalization, and admission to intensive care unit. The sample size allows detection of a 33% relative risk reduction in the primary outcome with 80% power.
Discussion: This trial assesses benefits and harms of a high inspiratory oxygen fraction, and the trial may be generalizable to a general surgical population undergoing laparotomy.
Trial registration: ClinicalTrials.gov identifier: NCT00364741.
Figures



References
-
- Babior BM. Oxygen-dependent microbial killing by phagocytes (first of two parts) N Engl J Med. 1978;298:659–668. - PubMed
-
- Allen DB, Maguire JJ, Mahdavian M, Wicke C, Marcocci L, Scheuenstuhl H, Chang M, Le AX, Hopf HW, Hunt TK. Wound hypoxia and acidosis limit neutrophil bacterial killing mechanisms. Arch Surg. 1997;132:991–996. - PubMed
-
- Hopf HW, Hunt TK, West JM, Blomquist P, Goodson WH, III, Jensen JA, Jonsson K, Paty PB, Rabkin JM, Upton RA, von Smitten K, Whitney JD. Wound tissue oxygen tension predicts the risk of wound infection in surgical patients. Arch Surg. 1997;132:997–1004. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
