

Recurrent varicella zoster virus myelopathy
- PMID: 18945446
- PMCID: PMC2828365
- DOI: 10.1016/j.jns.2008.09.025
Recurrent varicella zoster virus myelopathy
Abstract
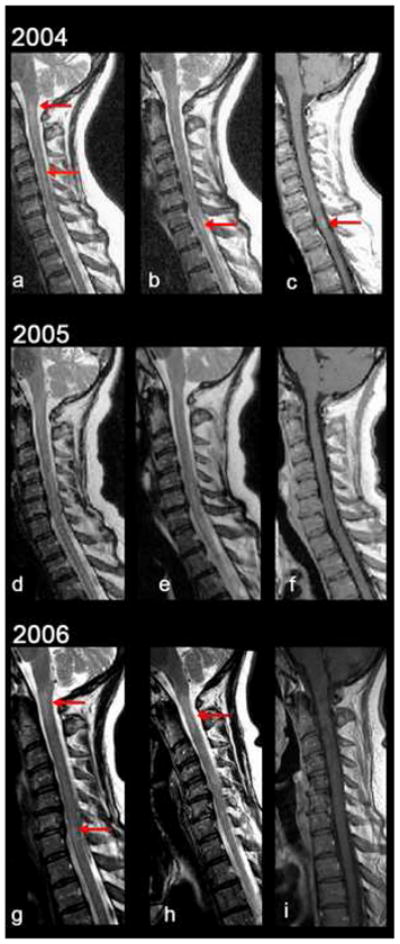
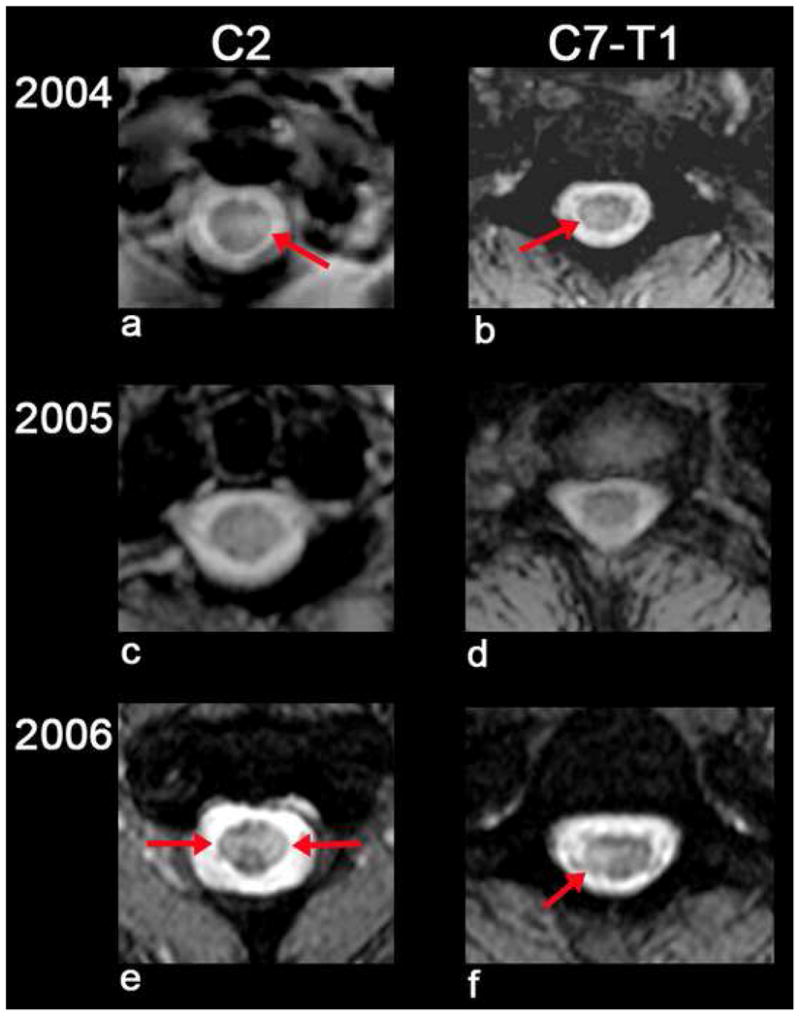
Myelopathy is an uncommon complication of VZV infection and may develop in the absence of rash. We report the rare recurrence of myelopathy in an immunocompetent adult who initially developed myelopathy after ophthalmic-distribution zoster. Recurrent myelopathy two years later caused by VZV was verified by the presence of new-onset clinical symptoms and signs consistent with myelopathy, new lesions in the spinal cord detected by MRI, and evidence of intrathecal synthesis of anti-VZV IgG antibody in CSF. After virological verification and antiviral therapy, myelopathy did not recur and anti-VZV IgG antibody could not be detected in CSF. In contrast to earlier cases of recurrent VZV myelopathy in immunocompetent adults that developed weeks to months after the first episode of myelopathy, this is the first instance of recurrence years later.
Figures
References
-
- Gilden DH, Beinleich BR, Rubinstien EM, Stommel E, Swenson R, Rubinstein D, Mahalingam R. Varicella-zoster virus myelitis: an expanding spectrum. Neurology. 1994;44:1818–23. - PubMed
-
- de Silva SM, Mark AS, Gilden DH, Mahalingam R, Balish M, Sandbrink F, Houff S. Zoster meyelitis: improvement with antiviral therapy in two cases. Neurology. 1996;47:929–31. - PubMed
-
- Orme HT, Smith AG, Nagel MA, Bert RJ, Mickelson TS, Gilden DH. VZV spinal cord infarction identified by diffusion-weighted MRI (DWI) Neurology. 2007;69:298–400. - PubMed
-
- Gilden DH, Lipton HL, Wolf JS, Akenbrandt W, Smith JE, Mahalingam R, Forghani B. Two patients with unusual forms of varicella-zoster virus vasculopathy. N Engl J Med. 2002;347:1500–3. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
