

Higher-risk periods for suicide among VA patients receiving depression treatment: prioritizing suicide prevention efforts
- PMID: 18945495
- PMCID: PMC2909461
- DOI: 10.1016/j.jad.2008.08.020
Higher-risk periods for suicide among VA patients receiving depression treatment: prioritizing suicide prevention efforts
Abstract
Background: Health systems with limited resources may have the greatest impact on suicide if their prevention efforts target the highest-risk treatment groups during the highest-risk periods. To date, few health systems have carefully segmented their depression treatment populations by level of risk and prioritized prevention efforts on this basis.
Methods: We conducted a retrospective cohort study of 887,859 VA patients receiving depression treatment between 4/1/1999 and 9/30/2004. We calculated suicide rates for five sequential 12-week periods following treatment events that health systems could readily identify: psychiatric hospitalizations, new antidepressant starts (>6 months without fills), "other" antidepressant starts, and dose changes. Using piecewise exponential models, we examined whether rates differed across time-periods. We also examined whether suicide rates differed by age-group in these periods.
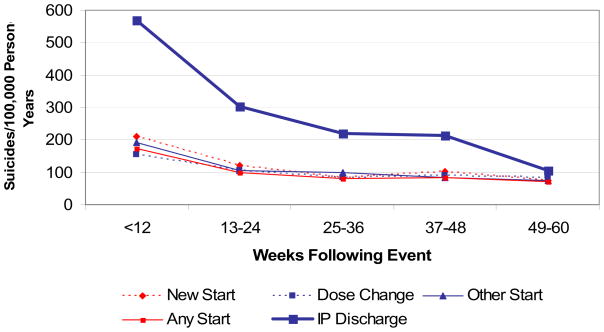
Results: Over all time-periods, the suicide rate was 114/100,000 person-years (95% CI; 108, 120). In the first 12-week periods, suicide rates were: 568/100,000 p-y (95% CI; 493, 651) following psychiatric hospitalizations; 210/100,000 p-y (95% CI; 187, 236) following new antidepressant starts; 193/100,000 p-y (95% CI; 167, 222) following other starts; and 154/100,000 p-y (95% CI; 133, 177) following dose changes. Suicide rates remained above the base rate for 48 weeks following hospital discharge and 12 weeks following antidepressant events. Adults aged 61-80 years were at highest risk in the first 12-week periods.
Conclusions: To have the greatest impact on suicide, health systems should prioritize prevention efforts following psychiatric hospitalizations. If resources allow, closer monitoring may also be warranted in the first 12 weeks following antidepressant starts, across all age-groups.
Figures
Similar articles
-
Service implications of providing intensive monitoring during high-risk periods for suicide among VA patients with depression.Psychiatr Serv. 2009 Apr;60(4):439-44. doi: 10.1176/ps.2009.60.4.439. Psychiatr Serv. 2009. PMID: 19339317 Free PMC article.
-
Who receives outpatient monitoring during high-risk depression treatment periods?J Am Geriatr Soc. 2010 May;58(5):908-13. doi: 10.1111/j.1532-5415.2010.02810.x. Epub 2010 Apr 14. J Am Geriatr Soc. 2010. PMID: 20406321 Free PMC article.
-
Antidepressant agents and suicide death among US Department of Veterans Affairs patients in depression treatment.J Clin Psychopharmacol. 2012 Jun;32(3):346-53. doi: 10.1097/JCP.0b013e3182539f11. J Clin Psychopharmacol. 2012. PMID: 22544011 Free PMC article.
-
Suicide risk factors among veterans: risk management in the changing culture of the Department of Veterans Affairs.J Ment Health Adm. 1997 Summer;24(3):350-8. doi: 10.1007/BF02832668. J Ment Health Adm. 1997. PMID: 9230576 Review.
-
Prevention of suicide and attempted suicide in Denmark. Epidemiological studies of suicide and intervention studies in selected risk groups.Dan Med Bull. 2007 Nov;54(4):306-69. Dan Med Bull. 2007. PMID: 18208680 Review.
Cited by
-
Predicting suicides after outpatient mental health visits in the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS).Mol Psychiatry. 2017 Apr;22(4):544-551. doi: 10.1038/mp.2016.110. Epub 2016 Jul 19. Mol Psychiatry. 2017. PMID: 27431294 Free PMC article.
-
Service implications of providing intensive monitoring during high-risk periods for suicide among VA patients with depression.Psychiatr Serv. 2009 Apr;60(4):439-44. doi: 10.1176/ps.2009.60.4.439. Psychiatr Serv. 2009. PMID: 19339317 Free PMC article.
-
Differences between veteran suicides with and without psychiatric symptoms.Am J Public Health. 2012 Mar;102 Suppl 1(Suppl 1):S125-30. doi: 10.2105/AJPH.2011.300415. Epub 2012 Jan 25. Am J Public Health. 2012. PMID: 22390586 Free PMC article.
-
Veteran-specific suicide prevention.Psychiatr Q. 2013 Jun;84(2):219-38. doi: 10.1007/s11126-012-9241-3. Psychiatr Q. 2013. PMID: 23011459 Review.
-
Editorial: The burden of stress and depression - new insight into faster and efficient treatment.Front Behav Neurosci. 2022 Aug 8;16:998307. doi: 10.3389/fnbeh.2022.998307. eCollection 2022. Front Behav Neurosci. 2022. PMID: 36004304 Free PMC article. No abstract available.
References
-
- Web-based Injury Statistics Query and Reporting System of the National Center for Injury Prevention and Control, Center for Disease Control and Prevention. available at http://www.cdc.gov/ncipc/wisqars.
-
- National Committee on Quality Assurance. State of Health Care Quality Report, Antidepressant Medication Management. available at http://www.ncqa.org/sohc2003/antidepressant_medication_manage.htm.
-
- American Psychiatric Association. Am J Psychiatry. Vol. 157. American Psychiatric Association; 2000. Practice guideline for the treatment of patients with major depressive disorder (revision) pp. 1–45. - PubMed
-
- American Psychiatric Association. Practice guideline for the assessment and treatment of patients with suicidal behaviors. Am J Psychiatry. 2003;160:1–60. - PubMed
-
- Cowper DC, Kubal JD, Maynard C, Hynes DM. A primer and comparative review of major US mortality databases. Ann Epidemiol. 2002;12:462–468. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
