

Quality of care and outcomes among patients with heart failure and chronic kidney disease: A Get With the Guidelines -- Heart Failure Program study
- PMID: 18946892
- PMCID: PMC2604122
- DOI: 10.1016/j.ahj.2008.05.028
Quality of care and outcomes among patients with heart failure and chronic kidney disease: A Get With the Guidelines -- Heart Failure Program study
Abstract
Background: Both heart failure (HF) and chronic kidney disease (CKD) are highly prevalent conditions that often coexist; however, the quality of care received by hospitalized patients with both is not known.
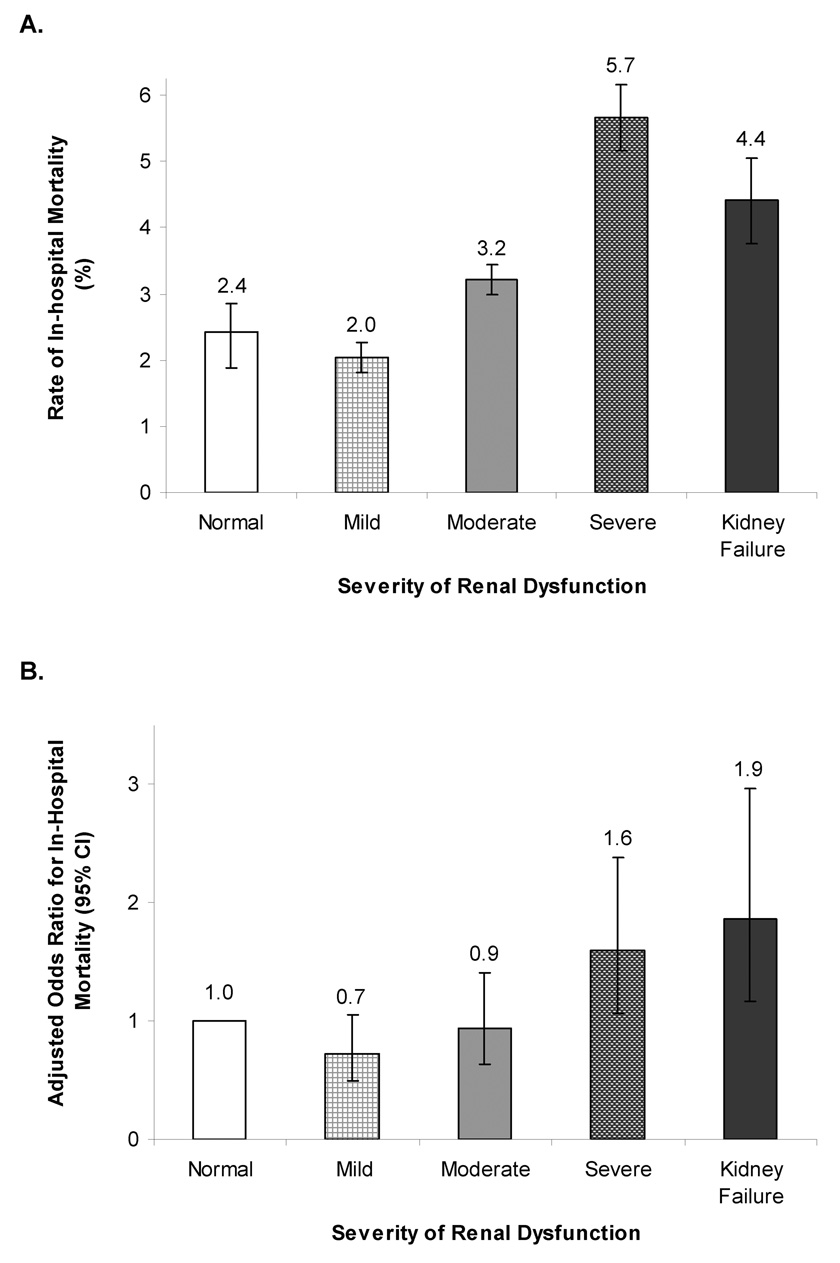
Methods: The Get With the Guidelines - HF registry and performance improvement program prospectively collects data on patients hospitalized with HF. Performance measures to improve treatment of patients with HF and inhospital mortality were examined by kidney function based on glomerular filtration rate (GFR) categorized as normal (GFR > or = 90), mild (60 < or = GFR < 90), moderate (30 < or = GFR < 60), severe (15 < or = GFR < 30), and kidney failure (GFR < 15 or dialysis).
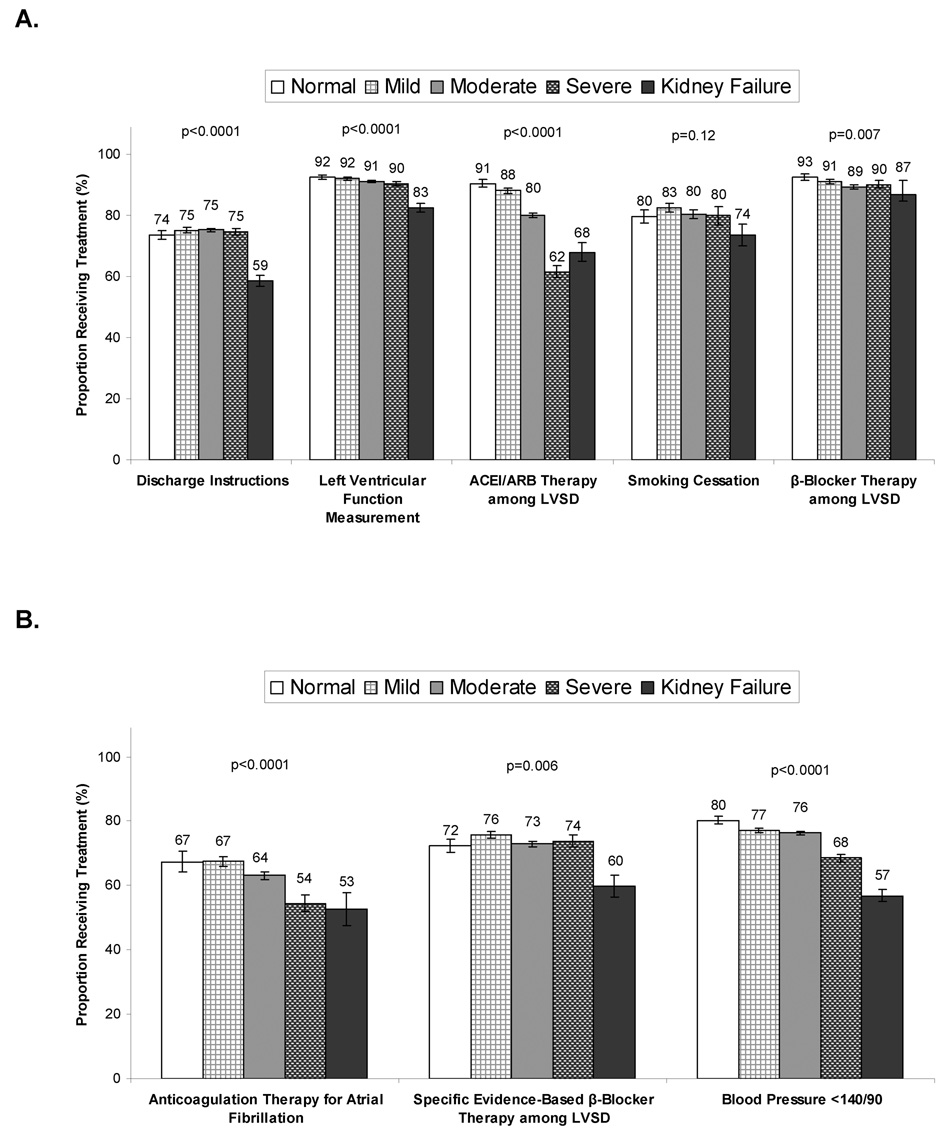
Results: Nearly two thirds of hospitalized patients with HF (15,560 patients from 137 hospitals) also had CKD: moderate CKD (43.9%), severe CKD (14.2%), and kidney failure (6.6%). Inpatient mortality was higher for patients with more severe renal dysfunction. Those with kidney failure were significantly less likely to receive nearly all guidelines-based therapies. In contrast, those with moderate or severe CKD often received similar care when compared with those with normal kidney function, except for lower use of angiotensin-converting enzyme inhibitors or receptor blockers (odds ratio 0.19 [0.13-0.28] and 0.47 [0.36-0.62], respectively) and lower proportions with blood pressure control (odds ratio 0.70 [0.58-0.85] and 0.52 [0.42-0.63], respectively).
Conclusions: In a large contemporary cohort of patients hospitalized with HF, we found that renal dysfunction was a highly prevalent comorbidity. Despite higher mortality rates, patients with increased severity of renal dysfunction were less likely to receive important guideline-recommended therapies. Further efforts are needed to improve the care of patients with HF and CKD.
Figures
References
-
- Association AH. Heart Disease and Stroke Statistics - 2007 Update. Dallas, TX: American Heart Association; 2007.
-
- Roger VL, Weston SA, Redfield MM, et al. Trends in heart failure incidence and survival in a community-based population. JAMA. 2004;292:344–350. - PubMed
-
- Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure): developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung Transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005;112:e154–e235. - PubMed
-
- Prevalence of chronic kidney disease and associated risk factors--United States, 1999–2004. MMWR. 2007;56:161–165. - PubMed
-
- Ezekowitz J, McAlister FA, Humphries KH, et al. The association among renal insufficiency, pharmacotherapy, and outcomes in 6,427 patients with heart failure and coronary artery disease. J Am Coll Cardiol. 2004;44:1587–1592. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
