

Transvenous removal of pacing and implantable cardiac defibrillating leads using single sheath mechanical dilatation and multiple venous approaches: high success rate and safety in more than 2000 leads
- PMID: 18948356
- PMCID: PMC2638651
- DOI: 10.1093/eurheartj/ehn461
Transvenous removal of pacing and implantable cardiac defibrillating leads using single sheath mechanical dilatation and multiple venous approaches: high success rate and safety in more than 2000 leads
Abstract
Aims: The aim of the present study was to describe a 10 years single-centre experience in pacing and defibrillating leads removal using an effective and safe modified mechanical dilatation technique.
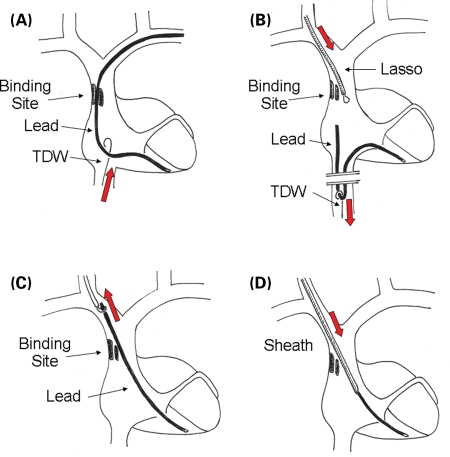
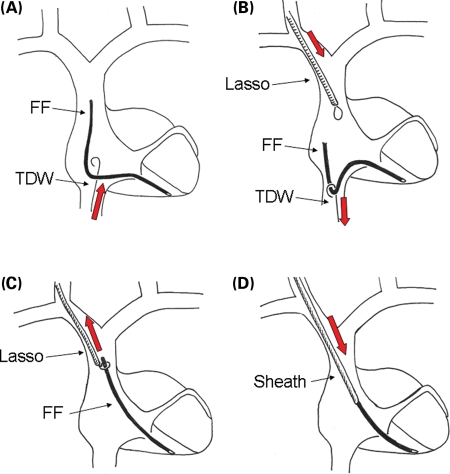
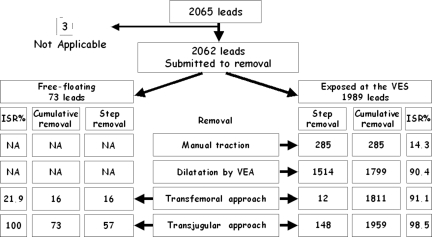
Methods and results: We developed a single mechanical dilating sheath extraction technique with multiple venous entry site approaches. We performed a venous entry site approach (VEA) in cases of exposed leads and an alternative transvenous femoral approach (TFA) combined with an internal transjugular approach (ITA) in the presence of very tight binding sites causing failure of VEA extraction or in cases of free-floating leads. We attempted to remove 2062 leads [1825 pacing and 237 implantable cardiac defibrillating (ICD) leads; 1989 exposed at the venous entry site and 73 free-floating] in 1193 consecutive patients. The VEA was effective in 1799 leads, the TFA in 28, and the ITA in 205; in the overall population, we completely removed 2032 leads (98.4%), partially removed 18 (0.9%), and failed to remove 12 leads (0.6%). Major complications were observed in eight patients (0.7%), causing three deaths (0.3%).
Conclusion: Mechanical single sheath extraction technique with multiple venous entry site approaches is effective, safe, and with a good cost effective profile for pacing and ICD leads removal.
Figures
References
-
- Furman S, Behrens M, Andrews C, Klementowicz P. Retained pacemaker leads. J Thoracic Cardiovasc Surg. 1987;94:770–772. - PubMed
-
- Rettig G, Doenecke P, Sen S, Volkmer I, Bette L. Complications with retained transvenous pacemaker electrodes. Am Heart J. 1979;98:587–594. - PubMed
-
- Parry G, Goudevenos J, Jameson S, Adams PG, Gold RG. Complications associated with retained pacemakers leads. Pacing Clin Electrophysiol. 1991;14:1251–1257. - PubMed
-
- Byrd CL, Schwartz SJ, Hedin NB, Goode LB, Feranot NE, Smith HJ. Intravascular lead extraction using locking stylets and sheaths. Pacing Clin Electrophysiol. 1990;13:1871–1875. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
