

Trends in malaria morbidity following the introduction of artesunate plus amodiaquine combination in M'lomp village dispensary, south-western Senegal
- PMID: 18950485
- PMCID: PMC2584070
- DOI: 10.1186/1475-2875-7-215
Trends in malaria morbidity following the introduction of artesunate plus amodiaquine combination in M'lomp village dispensary, south-western Senegal
Abstract
Background: In Thailand, South Africa and Zanzibar, a decrease in malaria morbidity was observed following the introduction of artemisinin-based combination therapy (ACT). In Senegal, therapeutic trials supervised the in vivo efficacy of artesunate plus amodiaquine from 1999 to 2005 at the M'lomp village dispensary. The trends in malaria morbidity in this village were evaluated from 2000 to 2002.
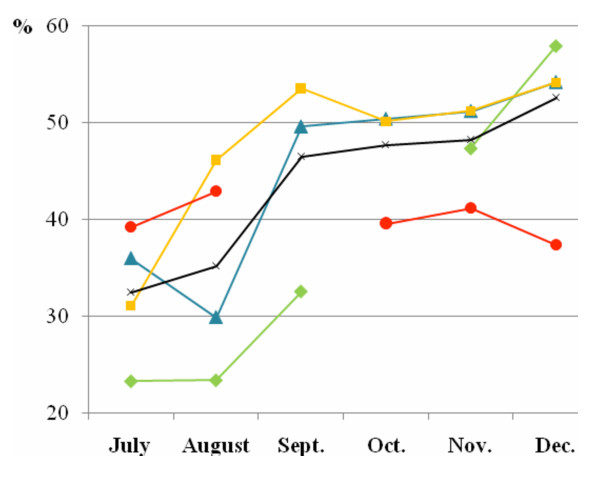
Methods: Each year, between July and December inclusive, fevers treated with antimalarials and slide-proven, uncomplicated malaria cases were collected from dispensary health records. Data were also collected in 1998, just prior to ACT introduction. Pearson's chi square tests and Student tests were used to compare two percentages or two means respectively (alpha = 0.05).
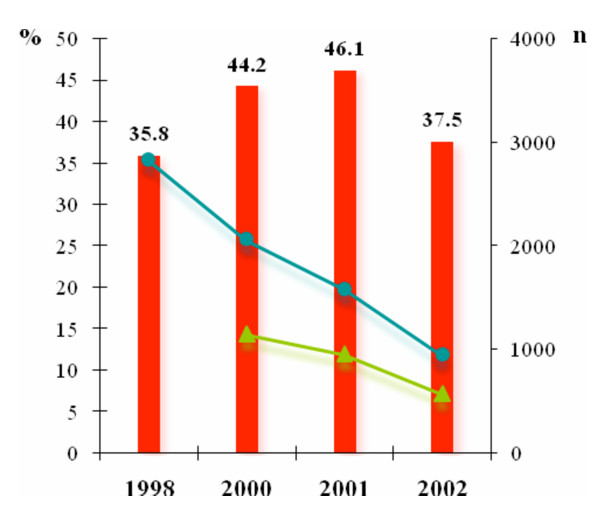
Results: Between 1998 and 2002, the total number of fevers treated with antimalarials and their repetitiveness progressively decreased: From 2824 to 945 fevers and from 17.6% to 9.7% (RR1998-2002 = 0.55; [0.44-0.69]; p < 0.0001) respectively. Considering uncomplicated malaria cases only, a decrease was observed in their total number between 2001 and 2002, from 953 to 570 cases. The incidence rate and repetitiveness also decreased. The incidence rate fell from 46.1% in 2001 to 37.5% in 2002 (p < 0.0001) and the repetitiveness decreased from 13.0% in 2000 to 6.6% in 2002 (RR2000-2002 = 0.51; [0.35-0.72]; p = 0.0001).
Conclusion: The percentage of uncomplicated malaria cases treated with ACT increased, from 18.9% in 2000 to 64.0% in 2002, making it tempting to conclude an impact on malaria morbidity. Nonetheless, the decline in incidence rate of uncomplicated malaria was slight and a lower recorded rainfall was reported in 2002 which could also explain this decline. The context in which ACT is introduced affects the impact on malaria morbidity. In M'lomp, in contrast to studies in Thailand, South Africa and Zanzibar, ACT coverage of malaria cases was low and no vector control measure was deployed. Moreover, the malaria transmission level is higher. In sub-Saharan countries, in order to optimize the impact on malaria morbidity, ACT deployment must be supported, on the one hand, by a strengthening of public health system to ensure a high ACT coverage and, on the other hand, by others measures, such vector control measures.
Figures
References
-
- WHO Antimalarial drug combination therapy. Report of a WHO Technical Consultation, WHO/CDS/RBM/200135.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
