

Obesity identified by discharge ICD-9 codes underestimates the true prevalence of obesity in hospitalized children
- PMID: 18950792
- PMCID: PMC4664085
- DOI: 10.1016/j.jpeds.2008.09.022
Obesity identified by discharge ICD-9 codes underestimates the true prevalence of obesity in hospitalized children
Abstract
Objectives: To define inpatient care of obese children with or without an obesity diagnosis.
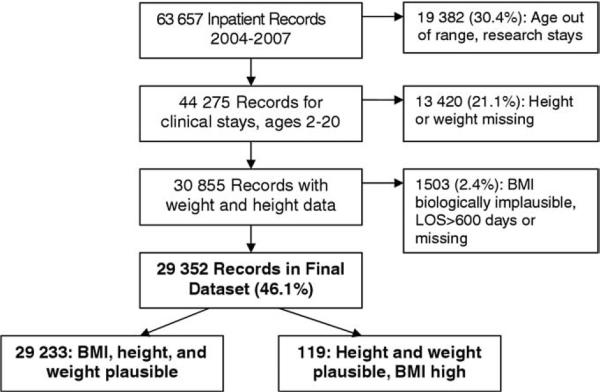
Study design: A total of 29,352 inpatient discharges (18,459 unique inpatients) from a tertiary children's hospital were analyzed. Body mass index (BMI) was calculated from measured height and weight. "Obesity" was defined as BMI >or=95th percentile by using Centers for Disease Control and Prevention 2000 growth charts. "Diagnosed obesity" was defined by primary, secondary or tertiary International Classification of Diseases, Ninth Revision codes for "obesity" or "overweight." Analyses controlled for multiple inpatient records per individual.
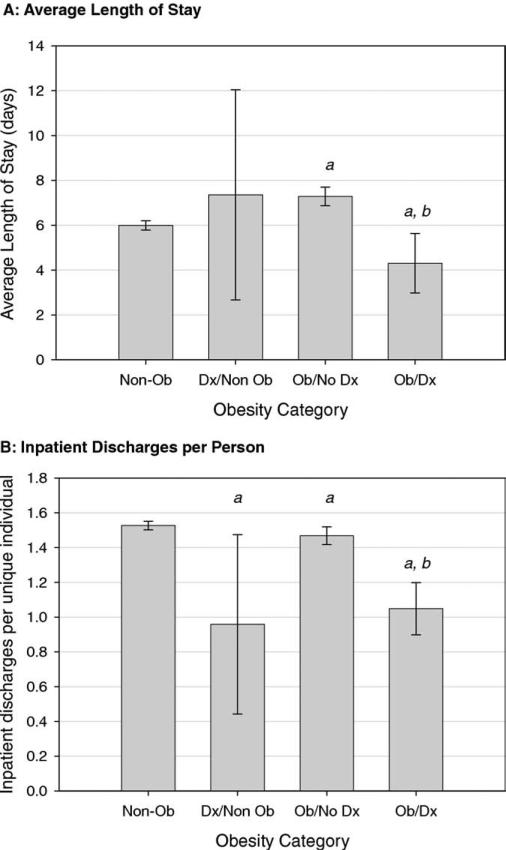
Results: A total of 5989 discharges from the hospital (20.4%) were associated with obesity, but only 512 discharges (1.7%) indicated obesity as a diagnosis. An obesity diagnosis identified only 5.5% of inpatient days for obese inpatients. Obese patients with an obesity diagnosis (Ob/Dx) had fewer hospital discharges per person and shorter lengths of stay than obese patients without an obesity diagnosis (Ob/No Dx). Patients with Ob/Dx had higher odds of mental health, endocrine, and musculoskeletal disorders than non-obese inpatients, but Ob/No Dx patients generally did not.
Conclusions: Inpatient obesity diagnoses underestimate inpatient utilization and misidentify patterns of care for obese children. Extreme caution is warranted when using obesity diagnoses to study healthcare utilization by obese children.
Figures
Comment in
-
Databases and diagnosis of obesity: pitfalls and potential of using ICD-9 codes.J Pediatr. 2009 Mar;154(3):315-7. doi: 10.1016/j.jpeds.2008.12.007. J Pediatr. 2009. PMID: 19874752 No abstract available.
References
-
- Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA. 2006;295:1549–55. - PubMed
-
- Heithoff KA, Cuffel BJ, Kennedy S, Peters J. The association between body mass and health care expenditures. Clin Ther. 1997;19:811–20. - PubMed
-
- Quesenberry CP, Jr, Caan B, Jacobson A. Obesity, health services use, and health care costs among members of a health maintenance organization. Arch Intern Med. 1998;158:466–72. - PubMed
-
- Wang G, Dietz WH. Economic burden of obesity in youths aged 6 to 17 years: 1979-1999. Pediatrics. 2002;109:e81. - PubMed
-
- Centers for Disease Control and Prevention [Dec 3, 2002];A SAS program for the CDC Growth Charts. Available at: www.cdc.gov/nccdphp/dnpa/growthcharts/sas.htm.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
