

Outcomes of a hospital-wide plan to improve care of comatose survivors of cardiac arrest
- PMID: 18951113
- PMCID: PMC2590640
- DOI: 10.1016/j.resuscitation.2008.08.014
Outcomes of a hospital-wide plan to improve care of comatose survivors of cardiac arrest
Abstract
Background: Therapeutic hypothermia (TH) improves outcomes in comatose survivors of cardiac arrest. Few hospitals have protocol-driven plans that include TH. We implemented a series of process interventions designed to increase TH use and improve outcomes in patients successfully resuscitated from out-of-hospital cardiac arrest (OHCA) or in-hospital cardiac arrest (IHCA).
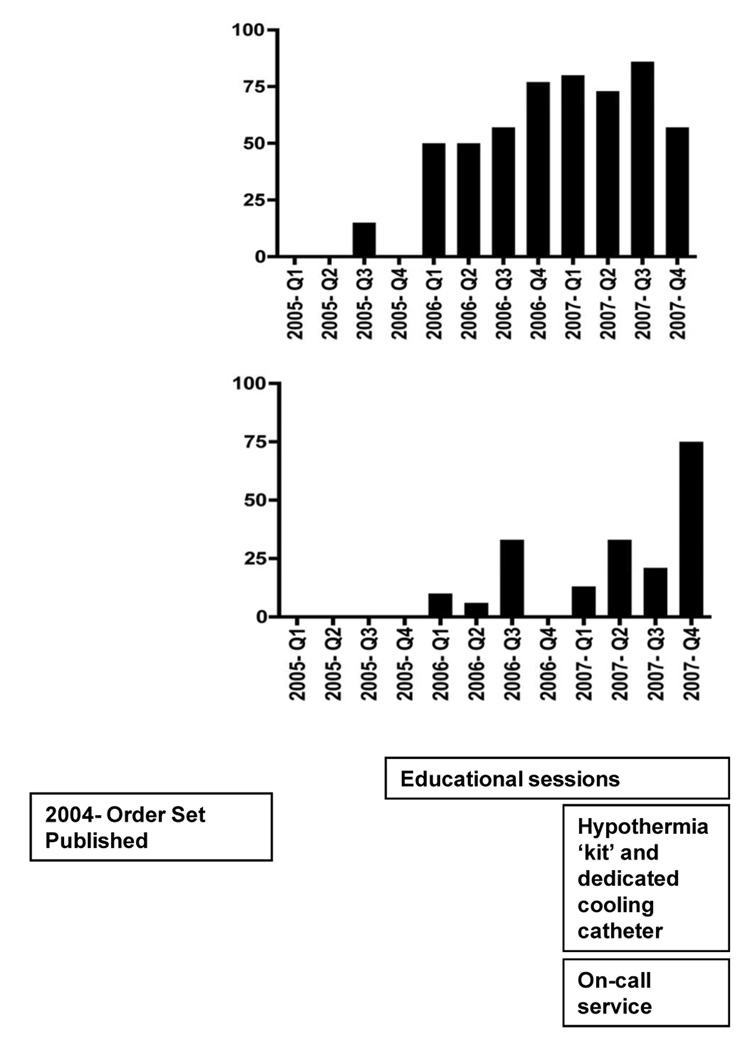
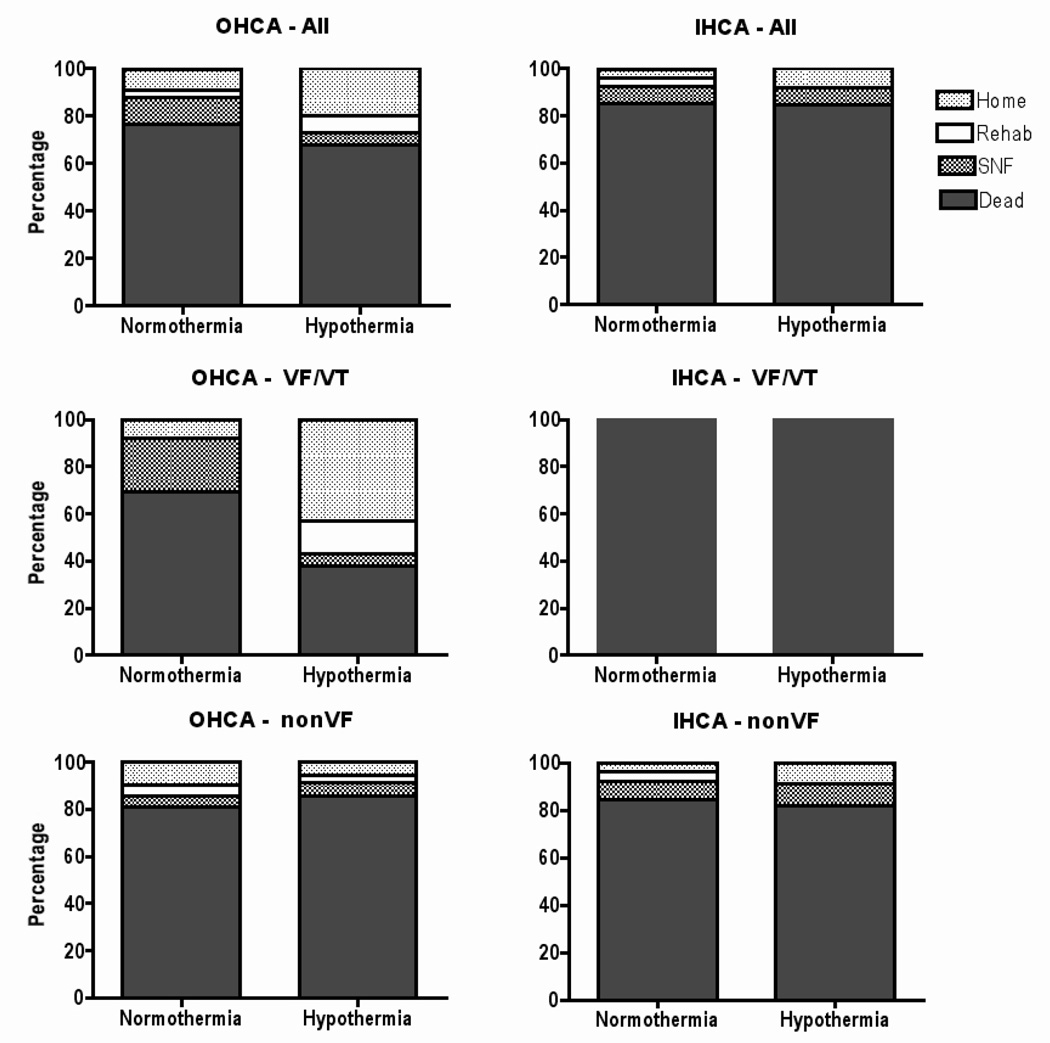
Methods and results: Linked interventions including a TH order sheet, verbal and written feedback to individual providers, an educational program, TH "kit" and on-call consultants to assist with patient care and hypothermia induction were implemented between January 1, 2005 and December 31, 2007 in a large, university-affiliated, tertiary care center. We then completed a retrospective review of all patients treated for cardiac arrest during the study period. Descriptive statistics, chi-squared analyses, or Fisher's exact test were used as appropriate. A p value <0.05 was considered significant. 135 OHCA patients and 106 IHCA patients were eligible for post-arrest care. TH use increased each year in the OHCA group (from 6% to 65% to 76%; p<0.001) and IHCA group (from 0% to 36% to 53%; p=.02). A good outcome was achieved in 21% and 8% of comatose patients with OHCA and IHCA, respectively. Patients with OHCA and ventricular dysrhythmia were more likely to have a good outcome with TH treatment than without it (good outcome in 57% vs. 8%; p=.005).
Conclusion: Implementing a series of aggressive interventions increased appropriate TH use and was associated with improved outcomes in our facility.
Figures


References
-
- Rosamond W, Flegal K, Furie K, et al. Heart disease and stroke statistics 2008 update. A report from the American Heart Association statistics committee and stroke statistics subcommittee. Circulation. 2008;117(4):e25–e146. - PubMed
-
- Nichol G, Stiell IG, Laupacis A, Pham B, DeMaio VJ, Wells GA. A cumulative meta-analysis of the effectiveness of defibrillator-capable emergency medical services for victims of out-of-hospital cardiac arrest. Ann Emerg Med. 1999;34(4 Pt 1):517–525. - PubMed
-
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report on 14720 cardiac arrests from the national registry of cardiopulmonary resuscitation. Resuscitation. 2003;58(3):297–308. - PubMed
-
- Langhalle A, Tyvold SS, Lexow K, Hapnes SA, Sunde K, Steen PA. In-hospital factors associated with improved outcome after out-of-hospital cardiac arrest. A comparison between four regions in Norway. Resuscitation. 2003;56(3):247–263. - PubMed
-
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346(8):549–556. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
