

Pilot study examining the combined use of pulsed dye laser and topical Imiquimod versus laser alone for treatment of port wine stain birthmarks
- PMID: 18951427
- PMCID: PMC2717850
- DOI: 10.1002/lsm.20716
Pilot study examining the combined use of pulsed dye laser and topical Imiquimod versus laser alone for treatment of port wine stain birthmarks
Abstract
Background and objective: The objective of this study was to improve port wine stain (PWS) therapeutic outcome in response to laser therapy. Our specific aim was to determine whether the combined use of pulsed dye laser (PDL) therapy and topical Imiquimod versus PDL alone can improve PWS therapeutic outcome.
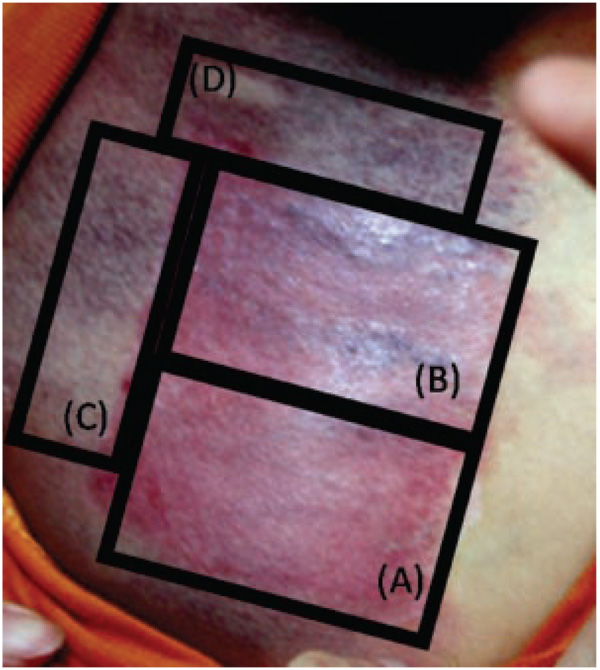
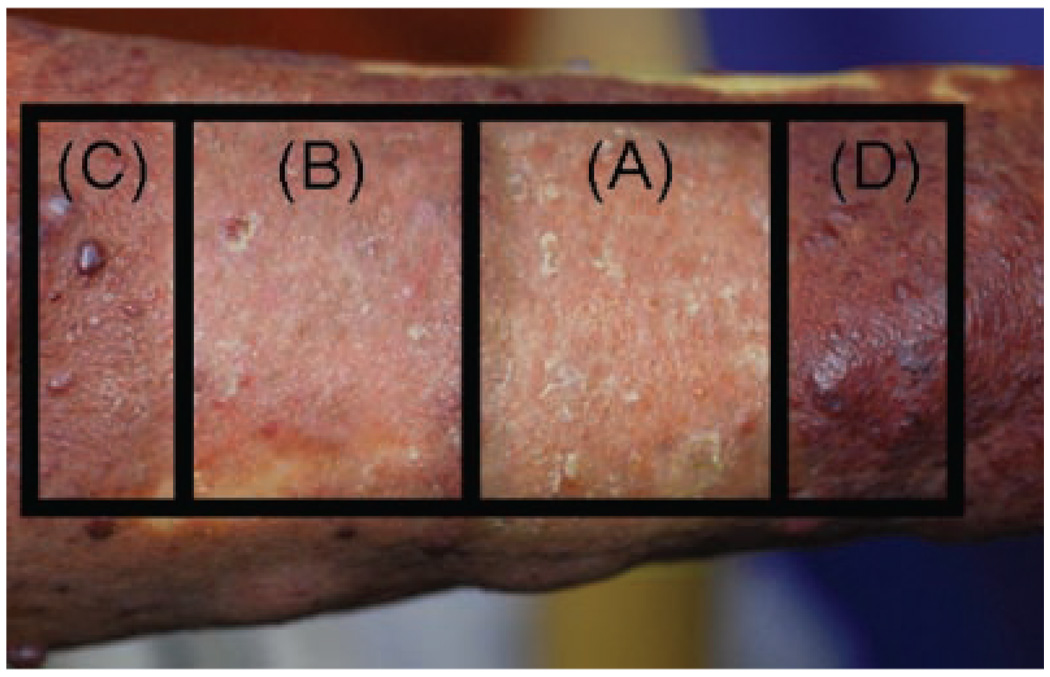
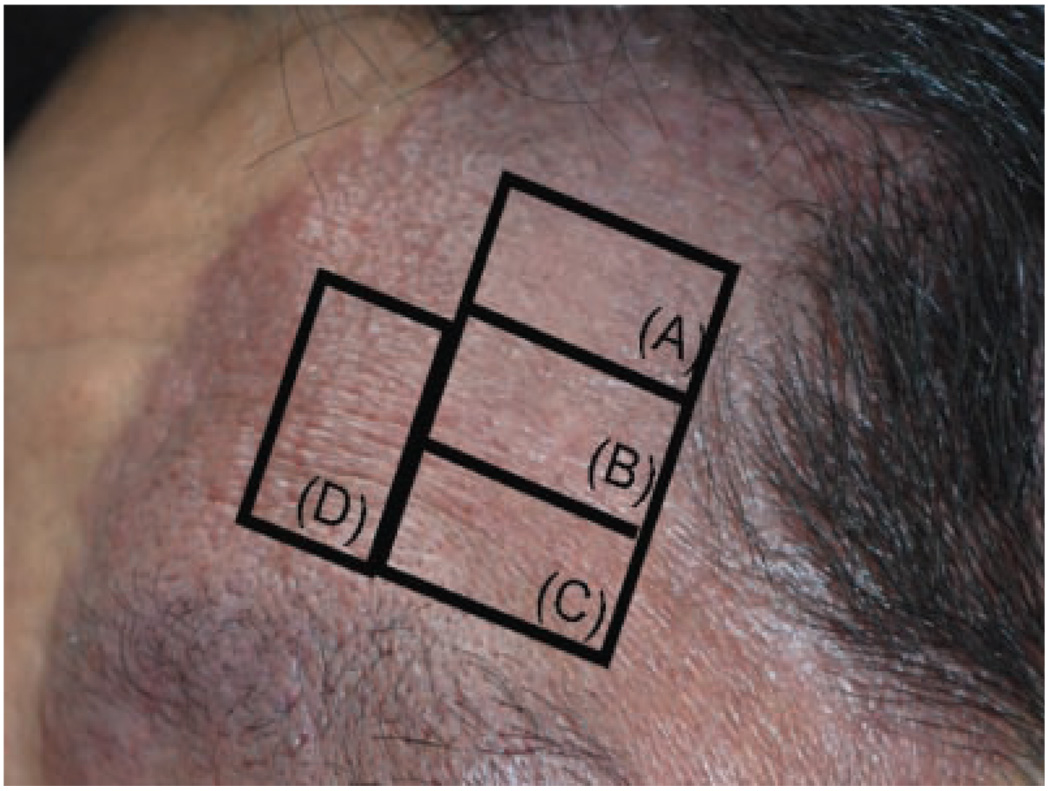
Study design/materials and methods: This pilot study involved a retrospective review of 20 subjects, all Asian, with PWS. Subject ages ranged between 3 and 56 years. Upon enrollment, three test sites were prospectively identified on each subject for treatment assignments to the following regimens: (A) PDL+Imiquimod; (B) PDL alone; and (C) Imiquimod alone. PDL test sites received a single treatment with a 585 nm wavelength; 1.5 milliseconds pulse duration; spot size 7 mm using a light dosage of 10 J/cm2 with cryogen spray cooling. For the PDL+Imiquimod and Imiquimod alone test sites, subjects were instructed to apply Imiquimod topically to the sites once daily for 1 month after PDL exposure. Subjects were followed-up at 1, 3, 6, and 12 months after PDL exposure to evaluate each of the three test sites. The primary efficacy measurement was the quantitative assessment of blanching responses as measured by a DermoSpectrometer to calculate the hemoglobin-index of each site at 1, 3, 6, and 12 months after PDL exposure. Subjects were also closely monitored for any adverse effects.
Results: Based on paired sample test analysis, there were clinically, and statistically significant, differences in blanching responses over time favoring PWS receiving PDL+Imiquimod as compared to either PDL or Imiquimod alone (P<0.05). At 12 months, it should be noted that there was some evidence of redarkening of PWS test sites treated by PDL+Imiquimod and PDL alone, presumably due to revascularization of blood vessels. However, based on comparison of the hemoglobin-indices determined at 1 and 12 months after PDL exposure, there was less revascularization of PWS test sites treated with PDL+Imiquimod as compared to PDL alone (P<0.05). Transient hyperpigmentation was noted in 10% (n = 2) and 40% (n = 8) of subjects on the PDL+Imiquimod and PDL alone test sites, respectively. On all sites, hyperpigmentation resolved spontaneously without medical intervention within 6 months. Permanent hypopigmentation or scarring was not observed on any test site.
Conclusion: Based on the results of this pilot study, PDL+Imiquimod resulted in superior blanching responses over time as compared to PDL alone for treatment of test sites on PWS lesions. Although the PDL+Imiquimod approach is intriguing, clinical validation in large PWS patient samples is required.
(c) 2008 Wiley-Liss, Inc.
Figures
References
-
- Mulliken JB, Young AR. Vascular Birthmarks-Hemangiomas and malformations. Saunders: Philadelphia: WB; 1988.
-
- Jacobs AH, Walton RG. The incidence of birthmarks in the neonate. Pediatrics. 1976;58:218–222. - PubMed
-
- Pratt AG. Birthmarks in infants. Arch Dermatol Syphilol. 1953;67:302–305. - PubMed
-
- Kalick SM. Toward an interdisciplinary psychology of appearances. Psychiatry. 1978;41:249–254. - PubMed
-
- Heller A, Rafman S, Svagulis I, Pless IB. Birth defects and psychosocial adjustment. Am J Dis Child. 1985;139:257–263. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
