

Cardiac catheterization is underutilized after in-hospital cardiac arrest
- PMID: 18951683
- PMCID: PMC2790918
- DOI: 10.1016/j.resuscitation.2008.07.015
Cardiac catheterization is underutilized after in-hospital cardiac arrest
Abstract
Background: Indications for immediate cardiac catheterization in cardiac arrest survivors without ST elevation myocardial infarction (STEMI) are uncertain as electrocardiographic and clinical criteria may be challenging to interpret in this population. We sought to evaluate rates of early catheterization after in-hospital ventricular fibrillation (VF) arrest and the association with survival.
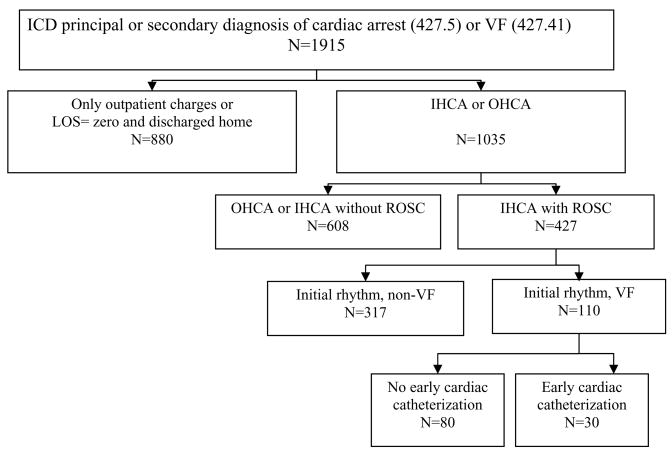
Methods: Using a billing database we retrospectively identified cases with an ICD-9 code of cardiac arrest (427.5) or VF (427.41). Discharge summaries were reviewed to identify in-hospital VF arrests. Rates of catheterization on the day of arrest were determined by identifying billing charges. Unadjusted analyses were performed using Chi-square, and adjusted analyses were performed using logistic regression.
Results: One hundred and ten in-hospital VF arrest survivors were included in the analysis. Cardiac catheterization was performed immediately or within 1 day of arrest in 27% (30/110) of patients and of these patients, 57% (17/30) successfully received percutaneous coronary intervention. Of those who received cardiac catheterization the indication for the procedure was STEMI or new left bundle branch block (LBBB) in 43% (13/30). Therefore, in the absence of standard ECG data suggesting acute myocardial infarction, 57% (17/30) received angiography. Patients receiving cardiac catheterization were more likely to survive than those who did not receive catheterization (80% vs. 54%, p<.05).
Conclusion: In patients receiving cardiac catheterization, more than half received this procedure for indications other than STEMI or new LBBB. Cardiac catheterization was associated with improved survival. Future recommendations need to be established to guide clinicians on which arrest survivors might benefit from immediate catheterization.
Conflict of interest statement
Figures
References
-
- Spaulding CM, Joly LM, Rosenberg A, et al. Immediate coronary angiography in survivors of out-of-hospital cardiac arrest. N Engl J Med. 1997;336:1629–33. - PubMed
-
- Davies MJ, Thomas A. Thrombosis and acute coronary-artery lesions in sudden cardiac ischemic death. N Engl J Med. 1984;310:1137–40. - PubMed
-
- Myerburg RJ, Kessler KM, Estes D, et al. Long-term survival after prehospital cardiac arrest: analysis of outcome during an 8 year study. Circulation. 1984;70:538–46. - PubMed
-
- Kahn JK, Glazier S, Swor R, Savas V, O’Neill WW. Primary coronary angioplasty for acute myocardial infarction complicated by out-of-hospital cardiac arrest. Am J Cardiol. 1995;75:1069–70. - PubMed
-
- Garot P, Lefevre T, Eltchaninoff H, et al. Six-month outcome of emergency percutaneous coronary intervention in resuscitated patients after cardiac arrest complicating ST-elevation myocardial infarction. Circulation. 2007;115:1354–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
