

Is adjuvant chemotherapy of benefit for postmenopausal women who receive endocrine treatment for highly endocrine-responsive, node-positive breast cancer? International Breast Cancer Study Group Trials VII and 12-93
- PMID: 18953651
- PMCID: PMC3589110
- DOI: 10.1007/s10549-008-0225-9
Is adjuvant chemotherapy of benefit for postmenopausal women who receive endocrine treatment for highly endocrine-responsive, node-positive breast cancer? International Breast Cancer Study Group Trials VII and 12-93
Abstract
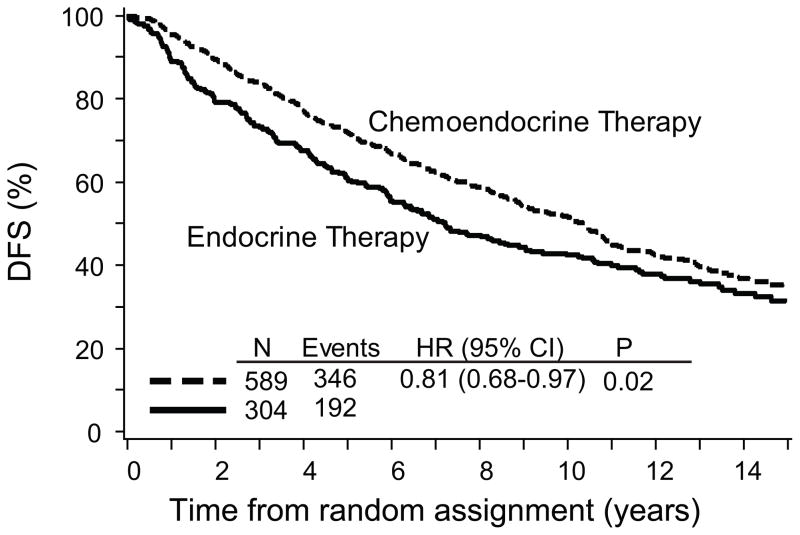
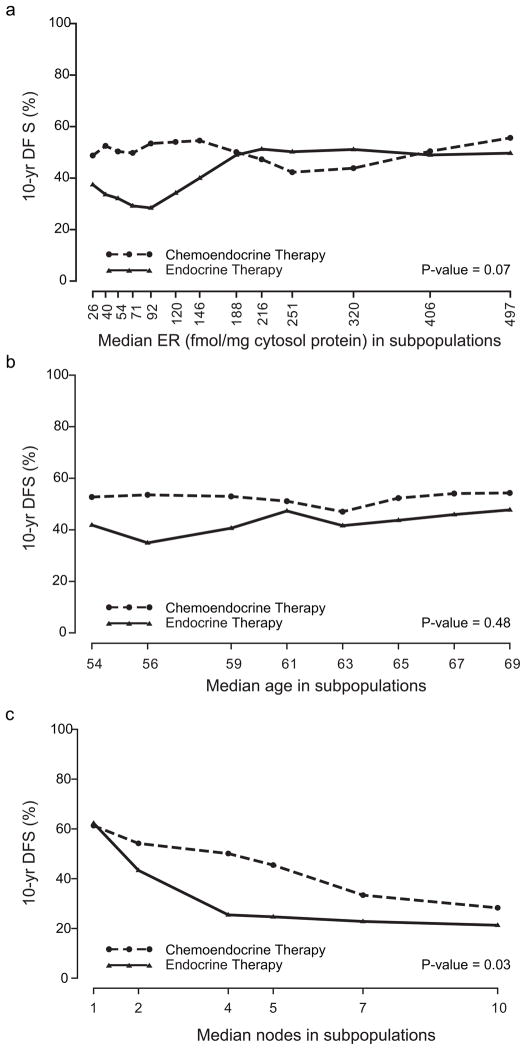
To compare the efficacy of chemoendocrine treatment with that of endocrine treatment (ET) alone for postmenopausal women with highly endocrine responsive breast cancer. In the International Breast Cancer Study Group (IBCSG) Trials VII and 12-93, postmenopausal women with node-positive, estrogen receptor (ER)-positive or ER-negative, operable breast cancer were randomized to receive either chemotherapy or endocrine therapy or combined chemoendocrine treatment. Results were analyzed overall in the cohort of 893 patients with endocrine-responsive disease, and according to prospectively defined categories of ER, age and nodal status. STEPP analyses assessed chemotherapy effect. The median follow-up was 13 years. Adding chemotherapy reduced the relative risk of a disease-free survival event by 19% (P = 0.02) compared with ET alone. STEPP analyses showed little effect of chemotherapy for tumors with high levels of ER expression (P = 0.07), or for the cohort with one positive node (P = 0.03). Chemotherapy significantly improves disease-free survival for postmenopausal women with endocrine-responsive breast cancer, but the magnitude of the effect is substantially attenuated if ER levels are high.
Figures
References
-
- Goldhirsch A, Wood WC, Gelber RD, et al. Progress and promise: highlights of the international expert consensus on the primary therapy of early breast cancer 2007. Ann Oncol. 2007;18:1133–1144. - PubMed
-
- Early Breast Cancer Trialists’ Collaborative Group. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365:1687–1717. - PubMed
-
- Goldhirsch A, Coates AS, Gelber RD, et al. First select the target: better choice of adjuvant treatments for breast cancer patients. Ann Oncol. 2006;17:1772–1776. - PubMed
-
- Crivellari D, Bonetti M, Castiglione-Gertsch M, et al. Burdens and benefits of adjuvant cyclophosphamide, methotrexate, and fluorouracil and tamoxifen for elderly patients with breast cancer: the International Breast Cancer Study Group trial VII. J Clin Oncol. 2000;18:1412–1422. - PubMed
