

Chemotherapy use for hormone receptor-positive, lymph node-negative breast cancer
- PMID: 18955448
- PMCID: PMC2651096
- DOI: 10.1200/JCO.2008.17.9705
Chemotherapy use for hormone receptor-positive, lymph node-negative breast cancer
Abstract
Purpose: To describe the frequency of chemotherapy use for hormone receptor (HR)-positive, lymph node (LN)-negative breast cancer from 1997 to 2004 at eight National Comprehensive Cancer Network institutions, to explore whether chemotherapy use varied over time and between institutions, and to identify factors associated with the decision to forego chemotherapy.
Patients and methods: Among women younger than age 70 years with HR-positive, LN-negative breast cancer measuring more than 1 cm, we analyzed the frequency of chemotherapy use on a yearly basis. A multivariable logistic regression model assessed the relationship between receipt of chemotherapy and year of diagnosis, institution, tumor features, and patient characteristics. Interaction terms were added to the model, and stratified analyses were conducted to further explore the determinants of chemotherapy use.
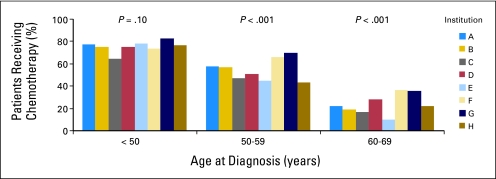
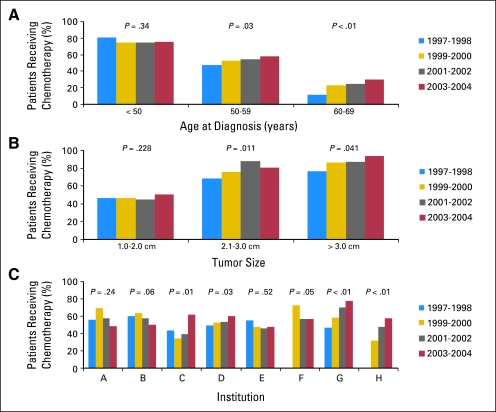
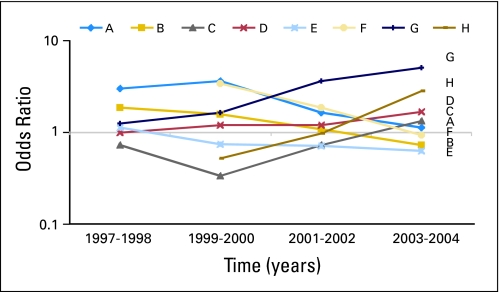
Results: Fifty-five percent of 3,190 women received chemotherapy. Chemotherapy use was less common for patients with 1.1- to 2-cm tumors than for patients tumors greater 2 cm (47% v 87%, respectively; P < .01) and for women age 60 to 69 years versus women younger than age 50 years (24% v 76%, respectively; P < .01). On multivariable analysis, predictors independently associated with receiving chemotherapy included larger tumor size, higher grade, human epidermal growth factor receptor 2 overexpression, younger age, and institution (P < .01 for all). Institutions exhibited dramatically different rates of chemotherapy use (from 46% to 65%) and patterns of change in chemotherapy use over time (from a 79% relative increase to a 22% relative decrease).
Conclusion: Although institutions seemed to agree that not all women with HR-positive, LN-negative breast cancer need chemotherapy, there did not seem to be consensus regarding which women should get chemotherapy. Only prospective randomized controlled trials will conclusively establish which subtypes of HR-positive, LN-negative breast cancer benefit from chemotherapy.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al: Cancer statistics, 2007. CA Cancer J Clin 57:43-66, 2007 - PubMed
-
- American Cancer Society: Breast cancer facts & figures 2005-2006. http://www.cancer.org/downloads/STT/CAFF2005BrF.pdf
-
- Fisher B, Dignam J, Wolmark N, et al: Tamoxifen and chemotherapy for lymph node-negative, estrogen receptor-positive breast cancer. J Natl Cancer Inst 89:1673-1682, 1997 - PubMed
-
- Mansour EG, Gray R, Shatila AH, et al: Survival advantage of adjuvant chemotherapy in high-risk node-negative breast cancer: Ten-year analysis—An intergroup study. J Clin Oncol 16:3486-3492, 1998 - PubMed
-
- Early Breast Cancer Trialists’ Collaborative Group: Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet 365:1687-1717, 2005 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
