

Primary and secondary kinase genotypes correlate with the biological and clinical activity of sunitinib in imatinib-resistant gastrointestinal stromal tumor
- PMID: 18955458
- PMCID: PMC2651076
- DOI: 10.1200/JCO.2007.15.7461
Primary and secondary kinase genotypes correlate with the biological and clinical activity of sunitinib in imatinib-resistant gastrointestinal stromal tumor
Abstract
Purpose: Most gastrointestinal stromal tumors (GISTs) harbor mutant KIT or platelet-derived growth factor receptor alpha (PDGFRA) kinases, which are imatinib targets. Sunitinib, which targets KIT, PDGFRs, and several other kinases, has demonstrated efficacy in patients with GIST after they experience imatinib failure. We evaluated the impact of primary and secondary kinase genotype on sunitinib activity.
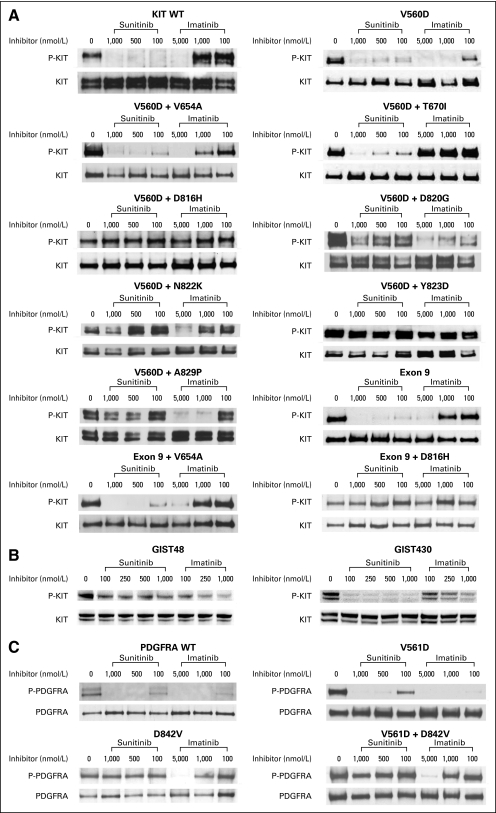
Patients and methods: Tumor responses were assessed radiologically in a phase I/II trial of sunitinib in 97 patients with metastatic, imatinib-resistant/intolerant GIST. KIT/PDGFRA mutational status was determined for 78 patients by using tumor specimens obtained before and after prior imatinib therapy. Kinase mutants were biochemically profiled for sunitinib and imatinib sensitivity.
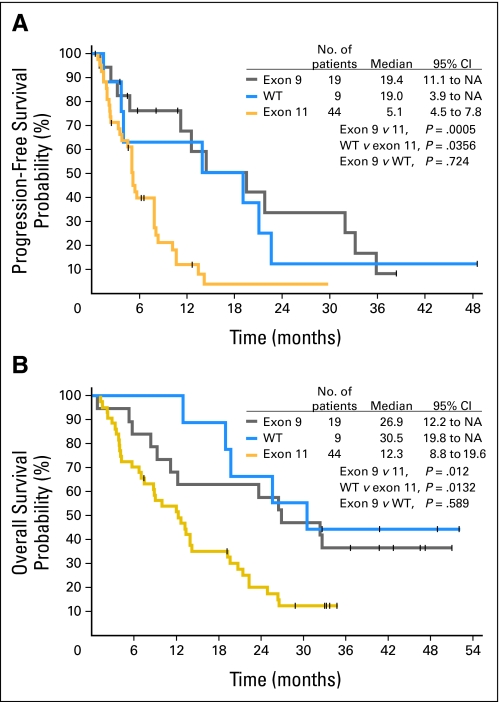
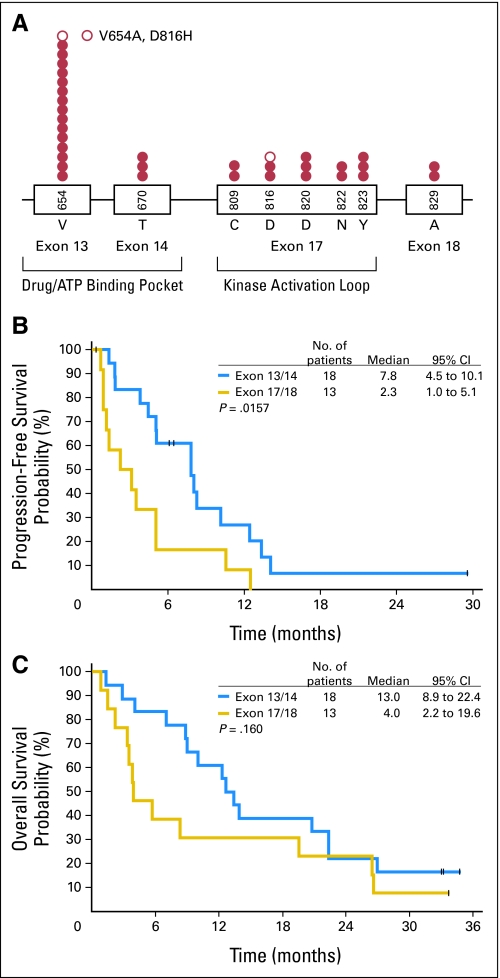
Results: Clinical benefit (partial response or stable disease for > or = 6 months) with sunitinib was observed for the three most common primary GIST genotypes: KIT exon 9 (58%), KIT exon 11 (34%), and wild-type KIT/PDGFRA (56%). Progression-free survival (PFS) was significantly longer for patients with primary KIT exon 9 mutations (P = .0005) or with a wild-type genotype (P = .0356) than for those with KIT exon 11 mutations. The same pattern was observed for overall survival (OS). PFS and OS were longer for patients with secondary KIT exon 13 or 14 mutations (which involve the KIT-adenosine triphosphate binding pocket) than for those with exon 17 or 18 mutations (which involve the KIT activation loop). Biochemical profiling studies confirmed the clinical results.
Conclusion: The clinical activity of sunitinib after imatinib failure is significantly influenced by both primary and secondary mutations in the predominant pathogenic kinases, which has implications for optimization of the treatment of patients with GIST.
Figures
Comment in
-
Prognosis, imatinib dose, and benefit of sunitinib in GIST: knowing the genotype.J Clin Oncol. 2008 Nov 20;26(33):5322-5. doi: 10.1200/JCO.2008.17.7725. Epub 2008 Oct 27. J Clin Oncol. 2008. PMID: 18955449 No abstract available.
References
-
- Corless CL, Schroeder A, Griffith D, et al: PDGFRA mutations in gastrointestinal stromal tumors: Frequency, spectrum and in vitro sensitivity to imatinib. J Clin Oncol 23:5357-5364, 2005 - PubMed
-
- Heinrich MC, Corless CL, Duensing A, et al: PDGFRA activating mutations in gastrointestinal stromal tumors. Science 299:708-710, 2003 - PubMed
-
- Debiec-Rychter M, Sciot R, Le Cesne A, et al: KIT mutations and dose selection for imatinib in patients with advanced gastrointestinal stromal tumours. Eur J Cancer 42:1093-1103, 2006 - PubMed
-
- Demetri GD, von Mehren M, Blanke CD, et al: Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med 347:472-480, 2002 - PubMed
-
- Verweij J, Casali PG, Zalcberg J, et al: Progression-free survival in gastrointestinal stromal tumours with high-dose imatinib: Randomised trial. Lancet 364:1127-1134, 2004 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
