

Cardiovascular outcomes in trials of oral diabetes medications: a systematic review
- PMID: 18955635
- PMCID: PMC2765722
- DOI: 10.1001/archinte.168.19.2070
Cardiovascular outcomes in trials of oral diabetes medications: a systematic review
Abstract
Background: A wide variety of oral diabetes medications are currently available for the treatment of type 2 diabetes mellitus, but it is unclear how these agents compare with respect to long-term cardiovascular risk. Our objective was to systematically examine the peer-reviewed literature on the cardiovascular risk associated with oral agents (second-generation sulfonylureas, biguanides, thiazolidinediones, and meglitinides) for treating adults with type 2 diabetes.
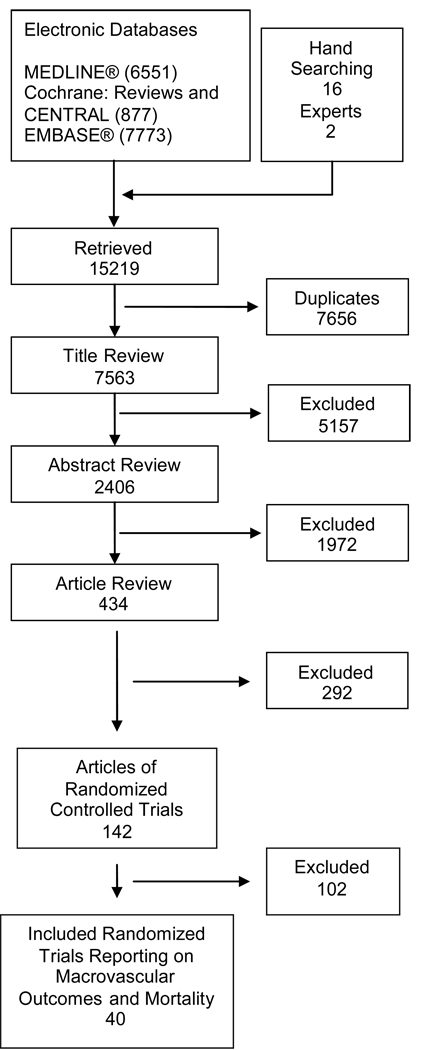
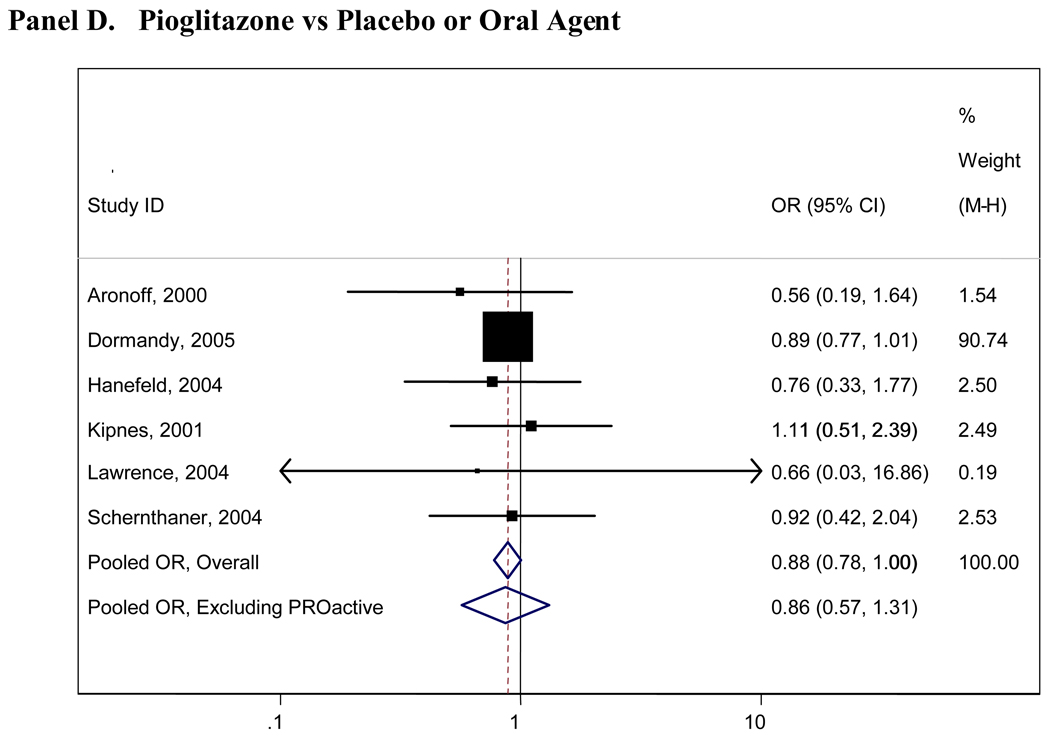
Methods: We searched MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials, from inception through January 19, 2006. Forty publications of controlled trials that reported information on cardiovascular events (primarily myocardial infarction and stroke) met our inclusion criteria. Using standardized protocols, 2 reviewers serially abstracted data from each article. Trials were first described qualitatively. For comparisons with 4 or more independent trials, results were pooled quantitatively using the Mantel-Haenszel method. Results are presented as odds ratios (ORs) and corresponding 95% confidence intervals (CIs).
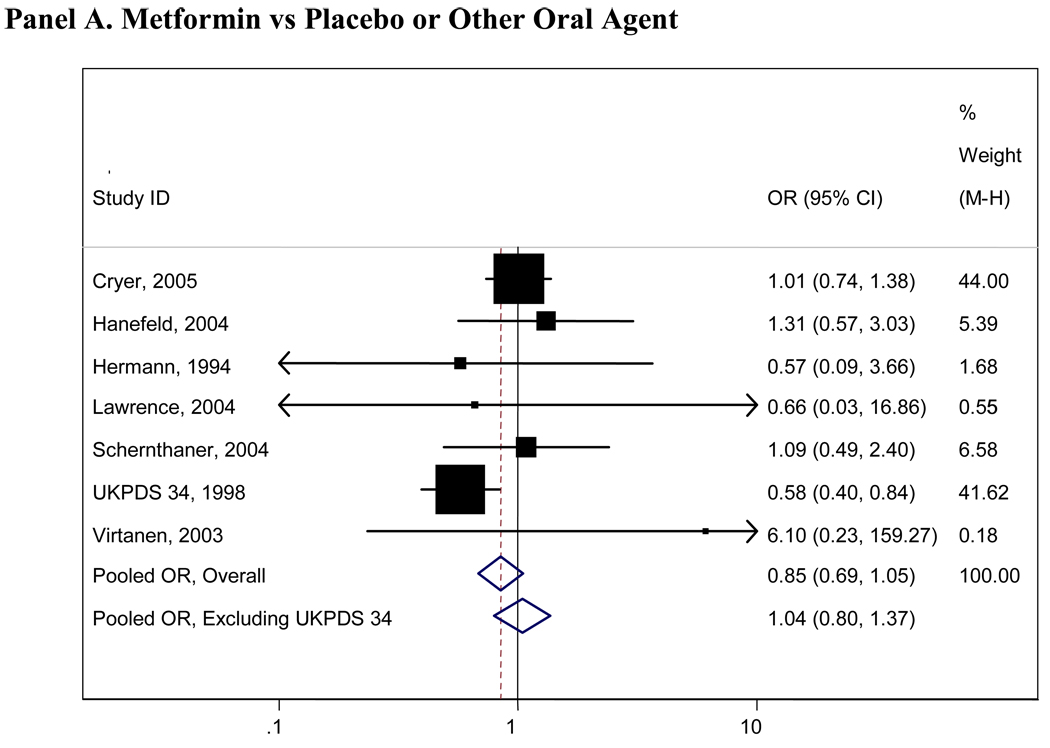
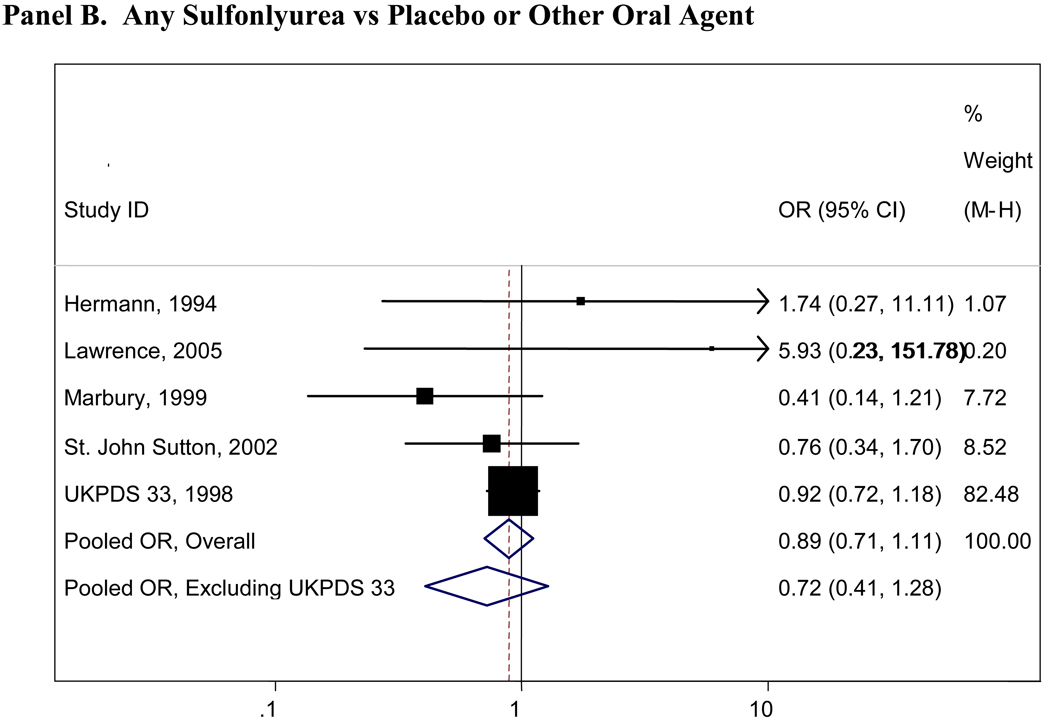
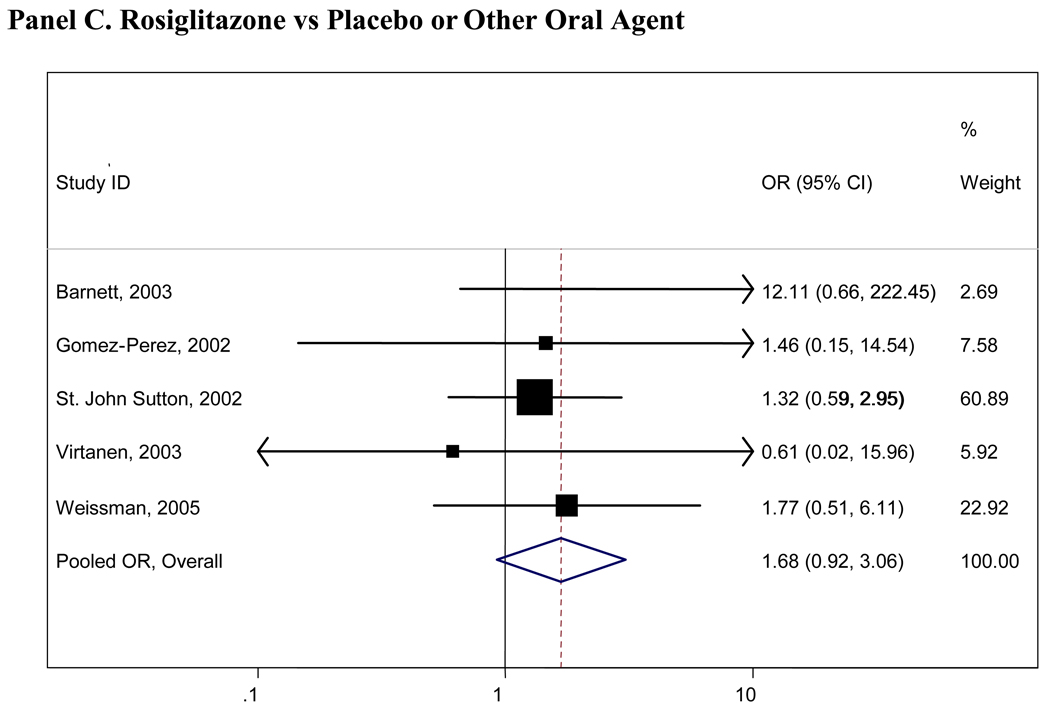
Results: Treatment with metformin hydrochloride was associated with a decreased risk of cardiovascular mortality (pooled OR, 0.74; 95% CI, 0.62-0.89) compared with any other oral diabetes agent or placebo; the results for cardiovascular morbidity and all-cause mortality were similar but not statistically significant. No other significant associations of oral diabetes agents with fatal or nonfatal cardiovascular disease or all-cause mortality were observed. When compared with any other agent or placebo, rosiglitazone was the only diabetes agent associated with an increased risk of cardiovascular morbidity or mortality, but this result was not statistically significant (OR, 1.68; 95% CI, 0.92-3.06).
Conclusions: Meta-analysis suggested that, compared with other oral diabetes agents and placebo, metformin was moderately protective and rosiglitazone possibly harmful, but lack of power prohibited firmer conclusions. Larger, long-term studies taken to hard end points and better reporting of cardiovascular events in short-term studies will be required to draw firm conclusions about major clinical benefits and risks related to oral diabetes agents.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Comment in
-
Glycemic management of type 2 diabetes: how tight is right and how to get there.Arch Intern Med. 2008 Oct 27;168(19):2064-6. doi: 10.1001/archinte.168.19.2064. Arch Intern Med. 2008. PMID: 18955633 No abstract available.
-
ACP Journal Club. Review: Metformin reduces risk for CV mortality compared with other oral diabetes drugs or placebo in type 2 diabetes.Ann Intern Med. 2009 Apr 21;150(8):JC4-8. doi: 10.7326/0003-4819-150-8-200904210-02008. Ann Intern Med. 2009. PMID: 19391221 No abstract available.
References
-
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352(9131):837–853. - PubMed
-
- Selvin E, Marinopoulos S, Berkenblit G, Rami T, Brancati FL, Powe NR, et al. Meta-analysis: glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann Intern Med. 2004;141(6):421–431. - PubMed
-
- Selvin E, Coresh J, Golden SH, Brancati FL, Folsom AR, Steffes MW. Glycemic Control and Coronary Heart Disease Risk in Persons With and Without Diabetes: The Atherosclerosis Risk in Communities Study. Archives of Internal Medicine. 2005;165(16):1910–1916. - PubMed
-
- Khaw KT, Wareham N, Bingham S, Luben R, Welch A, Day N. Association of hemoglobin A1c with cardiovascular disease and mortality in adults: the European prospective investigation into cancer in Norfolk. Ann Intern Med. 2004;141(6):413–420. - PubMed
