

The HAT Score: a simple grading scale for predicting hemorrhage after thrombolysis
- PMID: 18955684
- PMCID: PMC2676961
- DOI: 10.1212/01.wnl.0000330297.58334.dd
The HAT Score: a simple grading scale for predicting hemorrhage after thrombolysis
Abstract
Objective: To develop a grading scale to predict the risk of intracerebral hemorrhage (ICH) and prognosis after treatment with IV tissue-plasminogen activator (t-PA) in patients with ischemic stroke.
Methods: We constructed a five-point scale based on NIH Stroke Scale score, extent of hypodensity on CT scan, serum glucose at baseline, and history of diabetes to predict the risk of hemorrhage after thrombolysis (HAT score). We evaluated the predictive ability of this scale, using c-statistics, in two independent cohorts: the t-PA treated group in the National Institute of Neurological Disorders and Stroke study, and consecutive patients treated with IV t-PA at our institution.
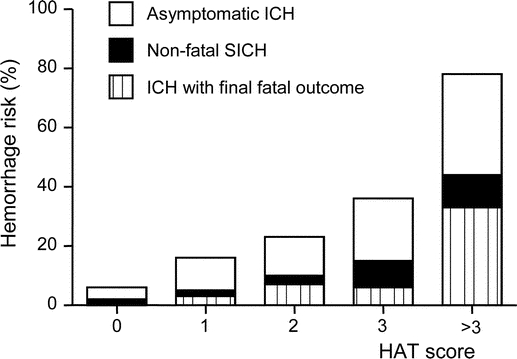
Results: The percentage of patients who developed any ICH after t-PA increased with higher scores in both cohorts. Collectively, the rate of any symptomatic ICH was 2% (0 point), 5% (1 point), 10% (2 points), 15% (3 points), and 44% (>3 points). The c-statistic was 0.72 (95% CI 0.65-0.79; p < 0.001) for all hemorrhages; 0.74 (0.63-0.84; p < 0.001) for symptomatic hemorrhages; and 0.79 (0.70-0.88; p < 0.001) for hemorrhages with final fatal outcome. Similar results were obtained when each cohort was analyzed separately. The score also reasonably predicted good (mRS < or = 2) (c-statistic 0.75; 0.69-0.80; p < 0.001) and catastrophic (mRS > or = 5) (0.78; 0.72-0.84; p < 0.001) functional outcomes on day 90 in the National Institute of Neurological Disorders and Stroke t-PA-treated patients.
Conclusions: The hemorrhage after thrombolysis (HAT) score is a practical, quick, and easy-to-perform scale that allows reasonable risk stratification of intracerebral hemorrhage after IV tissue-plasminogen activator (t-PA). However, the prognostic value of this scale and its use to predict the net benefit from t-PA needs to be refined and prospectively confirmed in a larger cohort of patients before it can be used in clinical decision-making.
Figures
References
-
- Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet 2004;363:768–774. - PubMed
-
- Douglas VC, Tong DC, Gillum LA, et al. Do the Brain Attack Coalition’s criteria for stroke centers improve care for ischemic stroke? Neurology 2005;64:422–427. - PubMed
-
- Tanne D, Kasner SE, Demchuk AM, et al. Markers of increased risk of intracerebral hemorrhage after intravenous recombinant tissue plasminogen activator therapy for acute ischemic stroke in clinical practice: the Multicenter rt-PA Stroke Survey. Circulation 2002;105:1679–1685. - PubMed
-
- Larrue V, von Kummer RR, Müller A, Bluhmki E. Risk factors for severe hemorrhagic transformation in ischemic stroke patients treated with recombinant tissue plasminogen activator: a secondary analysis of the European-Australasian Acute Stroke Study (ECASS II). Stroke 2001;32:438–441. - PubMed
-
- Demchuk AM, Morgenstern LB, Krieger DW, et al. Serum glucose level and diabetes predict tissue plasminogen activator-related intracerebral hemorrhage in acute ischemic stroke. Stroke 1999;30:34–39. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources