

Trends in adherence to secondary prevention medications in elderly post-myocardial infarction patients
- PMID: 18956426
- PMCID: PMC2680489
- DOI: 10.1002/pds.1671
Trends in adherence to secondary prevention medications in elderly post-myocardial infarction patients
Abstract
Background: Poor levels of medication adherence for patients with coronary heart disease (CHD) have been documented but it is unclear whether adherence has improved over time.
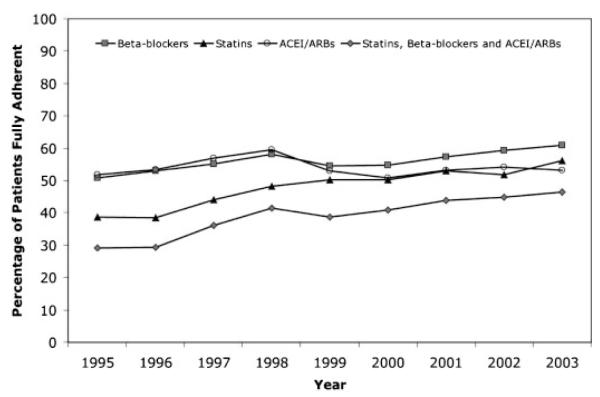
Methods: We assembled a retrospective cohort of lower-income Medicare beneficiaries who were discharged from the hospital after their first acute myocardial infarction (MI) between 1 January 1995 and 31 December 2003. For patients prescribed a statin, ACEI/ARB, beta-blocker, and all 3 of these medications after the hospital discharge, we evaluated medication adherence by determining the proportion of days covered (PDC) for each medication in the subsequent year.
Results: Our cohort consisted of a total of 33 646 patients. Adherence rates for statins and beta-blockers, but not ACEI/ARB, increased significantly over time but remained suboptimal. For example, among those patients that received a statin after discharge, 38.6% were fully adherent with therapy in 1995 in contrast to 56.2% in 2003 (p value for trend<0.001). Of patients prescribed all 3 of statin, beta-blocker, and ACEI/ARB, 29.1% and 46.4% were fully adherent in 1995 and 2003, respectively (p value for trend<0.001).
Conclusions: Our analysis demonstrates statistically significant but modest improvements in medication adherence for statins and beta-blockers, but not ACEI/ARBs, among patients discharged from hospital after acute MI. Despite these improvements, rates of non-adherence to these highly effective therapies remain extremely high. Given the health and economic consequences of non-adherence, the development of cost-effective strategies to improve medication adherence should be a clear priority.
Copyright (c) 2008 John Wiley & Sons, Ltd.
Figures
References
-
- Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: Part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation. 2001;104:2746–2753. - PubMed
-
- American Heart Association . Heart Disease and Stroke Statistics—2006 Uptake. Dallas:
-
- Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278. - PubMed
-
- Lopez-Sendon J, Swedberg K, McMurray J, et al. Expert consensus document on angiotensin converting enzyme inhibitors in cardiovascular disease. The task force on ACE-inhibitors of the European Society of Cardiology. Eur Heart J. 2004;25:1454–1470. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
