

Oral disposition index predicts the development of future diabetes above and beyond fasting and 2-h glucose levels
- PMID: 18957530
- PMCID: PMC2628704
- DOI: 10.2337/dc08-1478
Oral disposition index predicts the development of future diabetes above and beyond fasting and 2-h glucose levels
Erratum in
- Diabetes Care. 2009 Jul;32(7):1355
Abstract
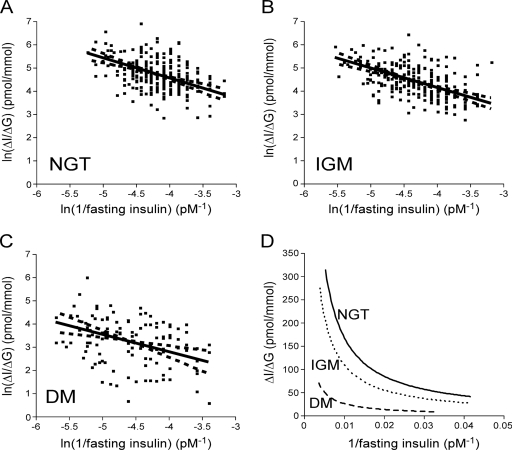
Objective: We sought to determine whether an oral disposition index (DI(O)) predicts the development of diabetes over a 10-year period. First, we assessed the validity of the DI(O) by demonstrating that a hyperbolic relationship exists between oral indexes of insulin sensitivity and beta-cell function.
Research design and methods: A total of 613 Japanese-American subjects (322 men and 291 women) underwent a 75-g oral glucose tolerance test (OGTT) at baseline, 5 years, and 10 years. Insulin sensitivity was estimated as 1/fasting insulin or homeostasis model assessment of insulin sensitivity (HOMA-S). Insulin response was estimated as the change in insulin divided by change in glucose from 0 to 30 min (DeltaI(0-30)/DeltaG(0-30)).
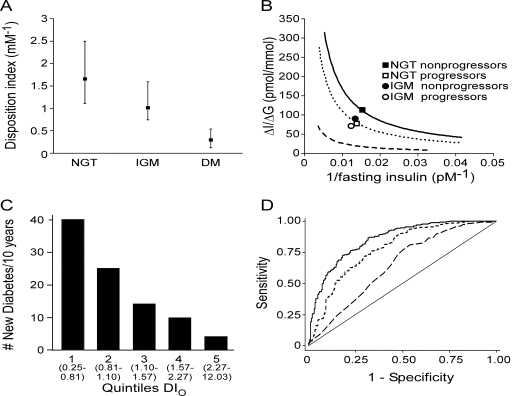
Results: DeltaI(0-30)/DeltaG(0-30) demonstrated a curvilinear relationship with 1/fasting insulin and HOMA-S with a left and downward shift as glucose tolerance deteriorated. The confidence limits for the slope of the log(e)-transformed estimates included -1 for DeltaI(0-30)/DeltaG(0-30) versus 1/fasting insulin for all glucose tolerance groups, consistent with a hyperbolic relationship. When HOMA-S was used as the insulin sensitivity measure, the confidence limits for the slope included -1 only for subjects with normal glucose tolerance (NGT) or impaired fasting glucose (IFG)/impaired glucose tolerance (IGT) but not diabetes. On the basis of this hyperbolic relationship, the product of DeltaI(0-30)/DeltaG(0-30) and 1/fasting insulin was calculated (DI(O)) and decreased from NGT to IFG/IGT to diabetes (P < 0.001). Among nondiabetic subjects at baseline, baseline DI(O) predicted cumulative diabetes at 10 years (P < 0.001) independent of age, sex, BMI, family history of diabetes, and baseline fasting and 2-h glucose concentrations.
Conclusions: The DI(O) provides a measure of beta-cell function adjusted for insulin sensitivity and is predictive of development of diabetes over 10 years.
Figures
Comment in
-
Oral disposition index predicts the development of future diabetes above and beyond fasting and 2-h glucose levels: response to Utzschneider et al.Diabetes Care. 2009 Jul;32(7):e86; author reply e87. doi: 10.2337/dc09-0537. Diabetes Care. 2009. PMID: 19564465 No abstract available.
References
-
- Kahn SE: The relative contributions of insulin resistance and β-cell dysfunction to the pathophysiology of type 2 diabetes. Diabetologia 46:3–19, 2003 - PubMed
-
- Kahn SE, Prigeon RL, McCulloch DK, Boyko EJ, Bergman RN, Schwartz MW, Neifing JL, Ward WK, Beard JC, Palmer JP, et al.: Quantification of the relationship between insulin sensitivity and β-cell function in human subjects: evidence for a hyperbolic function. Diabetes 42:1663–1672, 1993 - PubMed
-
- Buchanan TA, Xiang AH, Peters RK, Kjos SL, Marroquin A, Goico J, Ochoa C, Tan S, Berkowitz K, Hodis HN, Azen SP: Preservation of pancreatic β-cell function and prevention of type 2 diabetes by pharmacological treatment of insulin resistance in high-risk Hispanic women. Diabetes 51:2796–2803, 2002 - PubMed
