

Clinical application of pacemakers in atrial tachyarrhythmias
- PMID: 18958264
- PMCID: PMC2572014
Clinical application of pacemakers in atrial tachyarrhythmias
Abstract
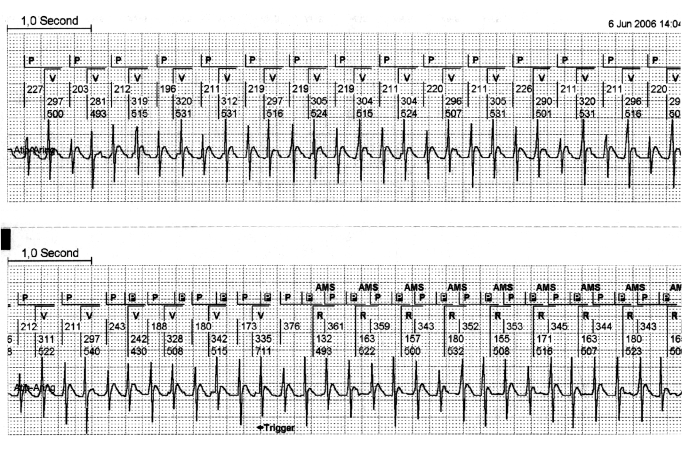
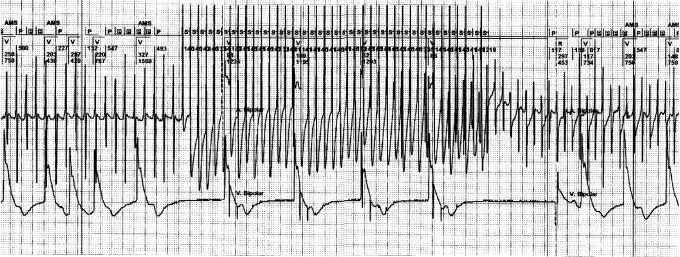
The diagnostic programmes of modern pacemakers have increased our knowledge of atrial tachyarrhythmias (ATAs) in chronically paced patients. These programmes also support the evaluation of the effects of pharmacological treatment of ATAs. The success of interruption and/or prevention of ATAs with pacemakers depends strongly on the diagnostic accuracy and the properties of the pacing algorithms, their individual programming and the site and configuration of the pacing leads. Atrial septum pacing can be beneficial in patients with paroxysmal atrial fibrillation and prolonged P wave duration. Recent large-scale studies on preventive and interruptive atrial pacing of ATAs show modestly positive or no results. Therefore, atrial pacing therapy for ATAs should be considered cautiously, serving as an adjuvant to pharmacological treatment rather than as a primary intervention. This also applies for pacing interventions for ATAs in cardiac resynchronisation therapy. The pacemaker algorithms for the detection of ATAs and atrial lead configuration are crucial for the success of pacemaker-mediated prevention or interruption of ATAs. The success of these interventions is dependant on future improvements of pacemaker technology. (Neth Heart J 2008;16(Suppl1):S20-S24.).
Keywords: atrial fibrillation; atrial pacing; atrial tachycardia; pace intervention; pace prevention.
Figures

References
-
- Israel CW, Barold SS. Pacemaker systems as implantable cardiac rhythm monitors. Am J Cardio l2001;88:442-5. - PubMed
-
- de Voogt WG, van Hemel NM, van de Bos AA, Koistinen J, Fast JH. Verification of pacemaker automatic mode switching for the detection of atrial fibrillation and atrial tachycardia with Holter recording. Europace 2006;8:950-61. - PubMed
-
- Israel CW, Barold SS. Failure of atrial flutter detection by a pacemaker with a dedicated atrial flutter detection algorithm. Pacing Clin Electrophysiol 2002;25:1274-7. - PubMed
-
- Goethals M, Timmermans W, Geelen P, Backers J, Brugada P. Mode switching failure during atrial flutter: the ‘2:1 lock-in’ phenomenon. Europace 2003;5:95-102. - PubMed
-
- de Voogt W, van Hemel N, Willems A, Visser J, Chitre Y, Bornzin G, et al. Far-field R-wave reduction with a novel lead design: experimental and human results. Pacing Clin Electrophysiol 2005;28:782-8. - PubMed
LinkOut - more resources
Full Text Sources