

Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety
- PMID: 18974308
- PMCID: PMC2702984
- DOI: 10.1056/NEJMoa0804633
Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety
Erratum in
- N Engl J Med. 2013 Jan 31;368(5):490
Abstract
Background: Anxiety disorders are common psychiatric conditions affecting children and adolescents. Although cognitive behavioral therapy and selective serotonin-reuptake inhibitors have shown efficacy in treating these disorders, little is known about their relative or combined efficacy.
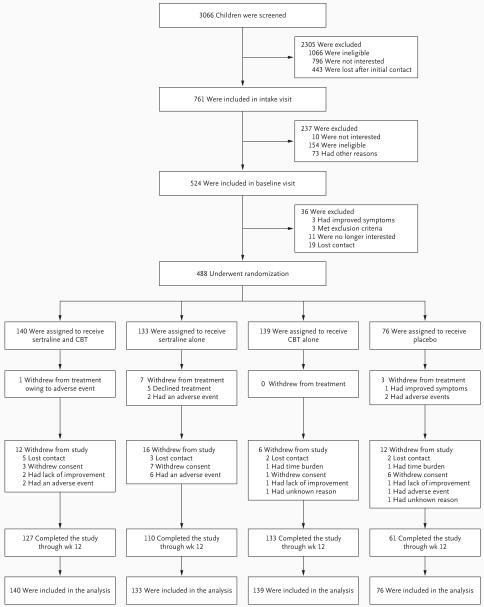
Methods: In this randomized, controlled trial, we assigned 488 children between the ages of 7 and 17 years who had a primary diagnosis of separation anxiety disorder, generalized anxiety disorder, or social phobia to receive 14 sessions of cognitive behavioral therapy, sertraline (at a dose of up to 200 mg per day), a combination of sertraline and cognitive behavioral therapy, or a placebo drug for 12 weeks in a 2:2:2:1 ratio. We administered categorical and dimensional ratings of anxiety severity and impairment at baseline and at weeks 4, 8, and 12.
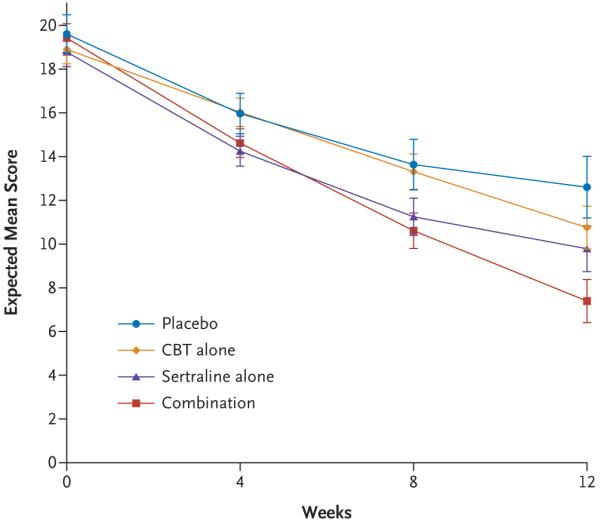
Results: The percentages of children who were rated as very much or much improved on the Clinician Global Impression-Improvement scale were 80.7% for combination therapy (P<0.001), 59.7% for cognitive behavioral therapy (P<0.001), and 54.9% for sertraline (P<0.001); all therapies were superior to placebo (23.7%). Combination therapy was superior to both monotherapies (P<0.001). Results on the Pediatric Anxiety Rating Scale documented a similar magnitude and pattern of response; combination therapy had a greater response than cognitive behavioral therapy, which was equivalent to sertraline, and all therapies were superior to placebo. Adverse events, including suicidal and homicidal ideation, were no more frequent in the sertraline group than in the placebo group. No child attempted suicide. There was less insomnia, fatigue, sedation, and restlessness associated with cognitive behavioral therapy than with sertraline.
Conclusions: Both cognitive behavioral therapy and sertraline reduced the severity of anxiety in children with anxiety disorders; a combination of the two therapies had a superior response rate. (ClinicalTrials.gov number, NCT00052078.)
2008 Massachusetts Medical Society
Figures
Comment in
-
Pediatric anxiety--underrecognized and undertreated.N Engl J Med. 2008 Dec 25;359(26):2835-6. doi: 10.1056/NEJMe0809401. N Engl J Med. 2008. PMID: 19109579 No abstract available.
-
Combination of cognitive behavioral therapy and sertraline is more effective than monotherapy for pediatric anxiety disorders.J Pediatr. 2009 May;154(5):775-6. doi: 10.1016/j.jpeds.2009.02.045. J Pediatr. 2009. PMID: 19364568 No abstract available.
-
A combination of cognitive-behavioural therapy and sertraline reduced anxiety in children more than either treatment alone.Evid Based Med. 2009 Jun;14(3):83. doi: 10.1136/ebm.14.3.83. Evid Based Med. 2009. PMID: 19483032 No abstract available.
-
Behavioral therapy, sertraline, or both in childhood anxiety.N Engl J Med. 2009 Jun 4;360(23):2475-6; author reply 2477. doi: 10.1056/NEJMc090139. N Engl J Med. 2009. PMID: 19494227 No abstract available.
-
Behavioral therapy, sertraline, or both in childhood anxiety.N Engl J Med. 2009 Jun 4;360(23):2476; author reply 2477. N Engl J Med. 2009. PMID: 19504760 No abstract available.
-
Behavioral therapy, sertraline, or both in childhood anxiety.N Engl J Med. 2009 Jun 4;360(23):2476; author reply 2477. N Engl J Med. 2009. PMID: 19504764 No abstract available.
-
Behavioral therapy, sertraline, or both in childhood anxiety.N Engl J Med. 2009 Jun 4;360(23):2476; author reply 2477. N Engl J Med. 2009. PMID: 19504765 No abstract available.
-
Short term CBT and sertraline, alone or in combination, reduce anxiety in children and adolescents.Evid Based Ment Health. 2009 Aug;12(3):88. doi: 10.1136/ebmh.12.3.88. Evid Based Ment Health. 2009. PMID: 19633256 No abstract available.
References
-
- Benjamin RS, Costello EJ, Warren M. Anxiety disorders in a pediatric sample. J Anxiety Disord. 1990;4:293–316.
-
- Birmaher B, Yelovich AK, Renaud J. Pharmacologic treatment for children and adolescents with anxiety disorders. Pediatr Clin North Am. 1998;45:1187–204. - PubMed
-
- Achenbach TM, Howell CT, McConaughy SH, et al. Six-year predictors of problems in a national sample of children and youth: I. Cross-informant syndromes. J Am Acad Child Adolesc Psychiatry. 1995;34:336–47. - PubMed
-
- Ferdinand RF, Verhulst FC. Psychopathology from adolescence into young adulthood: an 8-year follow-up study. Am J Psychiatry. 1995;152:1586–94. - PubMed
-
- Pine DS, Cohen P, Gurley D, Brook J, Ma Y. The risk for early-adulthood anxiety and depressive disorders in adolescents with anxiety and depressive disorders. Arch Gen Psychiatry. 1998;55:56–64. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- K23 MH075843/MH/NIMH NIH HHS/United States
- U01 MH064107/MH/NIMH NIH HHS/United States
- U01 MH64003/MH/NIMH NIH HHS/United States
- U01 MH064092/MH/NIMH NIH HHS/United States
- U01 MH064089/MH/NIMH NIH HHS/United States
- U01 MH064088/MH/NIMH NIH HHS/United States
- U01 MH063747/MH/NIMH NIH HHS/United States
- U01 MH64092/MH/NIMH NIH HHS/United States
- L40 MH072315/MH/NIMH NIH HHS/United States
- U01 MH64088/MH/NIMH NIH HHS/United States
- U01 MH064003/MH/NIMH NIH HHS/United States
- U01 MH63747/MH/NIMH NIH HHS/United States
- U01 MH64107/MH/NIMH NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical