

Differential metabolic effects of pravastatin and simvastatin in hypercholesterolemic patients
- PMID: 18977478
- PMCID: PMC2751605
- DOI: 10.1016/j.atherosclerosis.2008.09.021
Differential metabolic effects of pravastatin and simvastatin in hypercholesterolemic patients
Abstract
Background: Lipophilic and hydrophilic statins have different effects on adiponectin and insulin resistance in experimental studies and different effects on the rate of onset of new diabetes in large scale clinical studies. Therefore, we hypothesized that simvastatin and pravastatin may have differential metabolic effects in hypercholesterolemic patients.
Methods: This was a randomized, single-blind, placebo-controlled, parallel study. Age, gender, and body mass index were matched. Forty-three patients were given placebo, simvastatin 20mg, or pravastatin 40 mg, respectively once daily for 2 months.
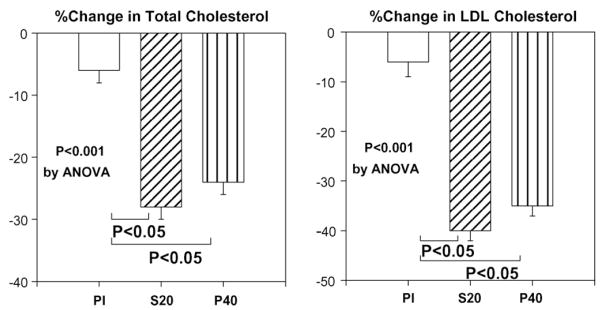
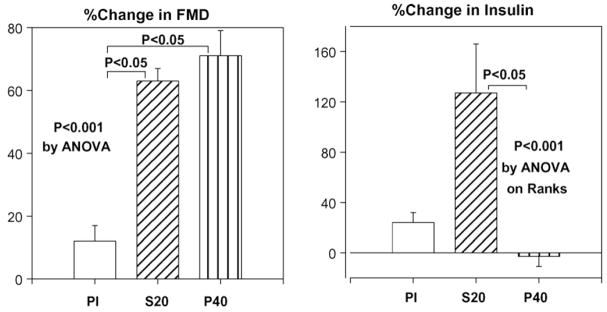
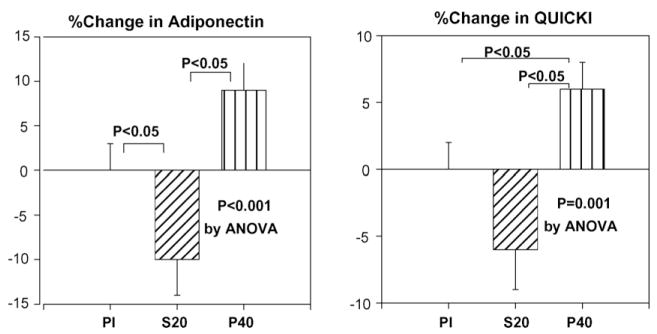
Results: Simvastatin and pravastatin therapy significantly changed lipoprotein levels and improved flow-mediated dilation after 2 months when compared with baseline (P<0.001) or placebo treatment (P<0.001 by ANOVA). Simvastatin therapy significantly increased insulin levels (mean % changes; 127%, P=0.014) and decreased plasma adiponectin levels (10%, P=0.012) and insulin sensitivity as assessed by QUICKI (6%, P=0.007) when compared with baseline. By contrast, pravastatin therapy did not significantly change insulin levels (-3%, P=0.437) but significantly increased plasma adiponectin levels (9%, P=0.011) and insulin sensitivity (6%, P=0.008) when compared with baseline. In addition, these effects of simvastatin were significant when compared with pravastatin (P<0.001 for insulin levels by ANOVA on Ranks, P<0.001 for adiponectin and P=0.001 for QUICKI by ANOVA). When compared with baseline, simvastatin significantly increased plasma leptin levels (35%, P=0.028), but pravastatin did not (1%, P=0.822).
Conclusions: Despite causing comparable changes in lipoprotein and endothelium-dependent dilation, simvastatin and pravastatin therapy had differential metabolic effects in hypercholesterolemic patients that may be clinically relevant.
Conflict of interest statement
All authors declare no conflict of interest.
Figures
Similar articles
-
Simvastatin improves flow-mediated dilation but reduces adiponectin levels and insulin sensitivity in hypercholesterolemic patients.Diabetes Care. 2008 Apr;31(4):776-82. doi: 10.2337/dc07-2199. Epub 2008 Jan 9. Diabetes Care. 2008. PMID: 18184901 Free PMC article. Clinical Trial.
-
Differential metabolic effects of rosuvastatin and pravastatin in hypercholesterolemic patients.Int J Cardiol. 2013 Jun 20;166(2):509-15. doi: 10.1016/j.ijcard.2011.11.028. Epub 2011 Dec 26. Int J Cardiol. 2013. PMID: 22204857 Clinical Trial.
-
Combination pravastatin and valsartan treatment has additive beneficial effects to simultaneously improve both metabolic and cardiovascular phenotypes beyond that of monotherapy with either drug in patients with primary hypercholesterolemia.Diabetes. 2013 Oct;62(10):3547-52. doi: 10.2337/db13-0566. Epub 2013 Jul 17. Diabetes. 2013. PMID: 23863812 Free PMC article. Clinical Trial.
-
Differential metabolic effects of distinct statins.Atherosclerosis. 2011 Mar;215(1):1-8. doi: 10.1016/j.atherosclerosis.2010.10.036. Epub 2010 Nov 2. Atherosclerosis. 2011. PMID: 21130454 Review.
-
Are statins created equal? Evidence from randomized trials of pravastatin, simvastatin, and atorvastatin for cardiovascular disease prevention.Am Heart J. 2006 Feb;151(2):273-81. doi: 10.1016/j.ahj.2005.04.003. Am Heart J. 2006. PMID: 16442888 Review.
Cited by
-
Do statins cause diabetes?Curr Diab Rep. 2013 Jun;13(3):381-90. doi: 10.1007/s11892-013-0368-x. Curr Diab Rep. 2013. PMID: 23456437 Review.
-
Comparison of simvastatin and metformin in treatment of polycystic ovary syndrome: prospective randomized trial.J Clin Endocrinol Metab. 2009 Dec;94(12):4938-45. doi: 10.1210/jc.2009-1674. Epub 2009 Nov 4. J Clin Endocrinol Metab. 2009. PMID: 19890022 Free PMC article. Clinical Trial.
-
Targeting Early Atherosclerosis: A Focus on Oxidative Stress and Inflammation.Oxid Med Cell Longev. 2019 Jul 1;2019:8563845. doi: 10.1155/2019/8563845. eCollection 2019. Oxid Med Cell Longev. 2019. PMID: 31354915 Free PMC article. Review.
-
Pharmacological effects of lipid-lowering drugs on circulating adipokines.World J Diabetes. 2010 Sep 15;1(4):116-28. doi: 10.4239/wjd.v1.i4.116. World J Diabetes. 2010. PMID: 21537437 Free PMC article.
-
Effects of simvastatin on serum adiponectin: a meta-analysis of randomized controlled trials.Lipids Health Dis. 2017 Mar 13;16(1):53. doi: 10.1186/s12944-017-0439-0. Lipids Health Dis. 2017. PMID: 28288631 Free PMC article.
References
-
- Sacks FM, Tonkin AM, Shepherd J, et al. Effect of pravastatin on coronary disease events in subgroups defined by coronary risk factors: the Prospective Pravastatin Pooling Project. Circulation. 2000;102:1893–900. - PubMed
-
- Kim J, Montagnani M, Koh KK, Quon MJ. Reciprocal relationships between insulin resistance and endothelial dysfunction: molecular and pathophysiological mechanisms. Circulation. 2006;113:1888–904. - PubMed
-
- Han SH, Quon MJ, Koh KK. Reciprocal relationships between abnormal metabolic parameters and endothelial dysfunction. Curr Opin Lipidol. 2007;18:58–65. - PubMed
-
- Muniyappa R, Montagnani M, Koh KK, Quon MJ. Cardiovascular actions of insulin. Endocr Rev. 2007;28:463–91. - PubMed
-
- Paolisso G, Barbagallo M, Petrella G, et al. Effects of simvastatin and atorvastatin administration on insulin resistance and respiratory quotient in aged dyslipidemic non-insulin dependent diabetic patients. Atherosclerosis. 2000;150:121–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
