

Pediatric cardiopulmonary resuscitation: advances in science, techniques, and outcomes
- PMID: 18977991
- PMCID: PMC2680157
- DOI: 10.1542/peds.2007-3313
Pediatric cardiopulmonary resuscitation: advances in science, techniques, and outcomes
Abstract
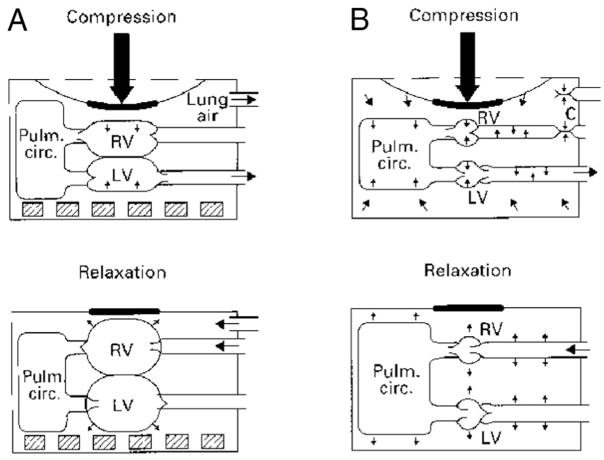
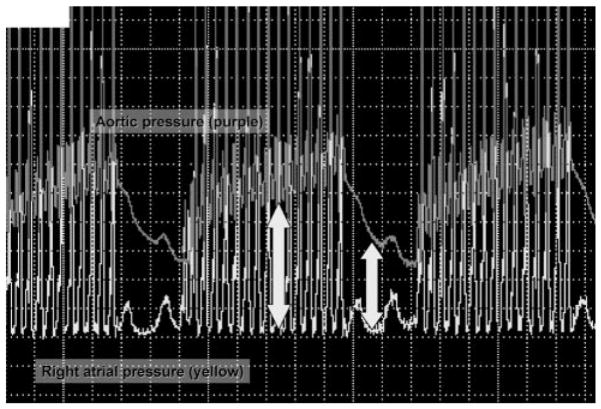
More than 25% of children survive to hospital discharge after in-hospital cardiac arrests, and 5% to 10% survive after out-of-hospital cardiac arrests. This review of pediatric cardiopulmonary resuscitation addresses the epidemiology of pediatric cardiac arrests, mechanisms of coronary blood flow during cardiopulmonary resuscitation, the 4 phases of cardiac arrest resuscitation, appropriate interventions during each phase, special resuscitation circumstances, extracorporeal membrane oxygenation cardiopulmonary resuscitation, and quality of cardiopulmonary resuscitation. The key elements of pathophysiology that impact and match the timing, intensity, duration, and variability of the hypoxic-ischemic insult to evidence-based interventions are reviewed. Exciting discoveries in basic and applied-science laboratories are now relevant for specific subpopulations of pediatric cardiac arrest victims and circumstances (eg, ventricular fibrillation, neonates, congenital heart disease, extracorporeal cardiopulmonary resuscitation). Improving the quality of interventions is increasingly recognized as a key factor for improving outcomes. Evolving training strategies include simulation training, just-in-time and just-in-place training, and crisis-team training. The difficult issue of when to discontinue resuscitative efforts is addressed. Outcomes from pediatric cardiac arrests are improving. Advances in resuscitation science and state-of-the-art implementation techniques provide the opportunity for further improvement in outcomes among children after cardiac arrest.
Figures
References
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA. 2006;295(1):50–57. - PubMed
-
- Chamnanvanakij S, Perlman JM. Outcome following cardiopulmonary resuscitation in the neonate requiring ventilatory assistance. Resuscitation. 2000;45(3):173–180. - PubMed
-
- Hintz SR, Benitz WE, Colby CE, Sheehan AM, Rycus P, Van Meurs KP. Utilization and outcomes of neonatal cardiac extracorporeal life support: 1996–2000. Pediatr Crit Care Med. 2005;6(1):33–38. - PubMed
-
- López-Herce J, Garcia C, Dominguez P, et al. Outcome of out-of-hospital cardiorespiratory arrest in children. Pediatr Emerg Care. 2005;21(12):807–815. - PubMed
-
- Meaney PA, Nadkarni VM, Cook EF, et al. Higher survival rates among younger patients after pediatric intensive care unit cardiac arrests. Pediatrics. 2006;118(6):2424–2433. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
