

Combined anteversion technique for total hip arthroplasty
- PMID: 18979146
- PMCID: PMC2600986
- DOI: 10.1007/s11999-008-0598-4
Combined anteversion technique for total hip arthroplasty
Abstract
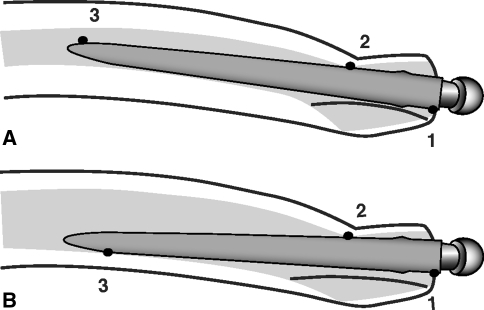
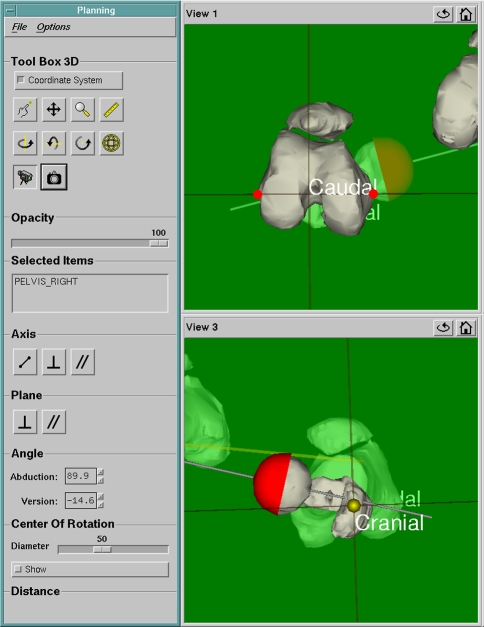
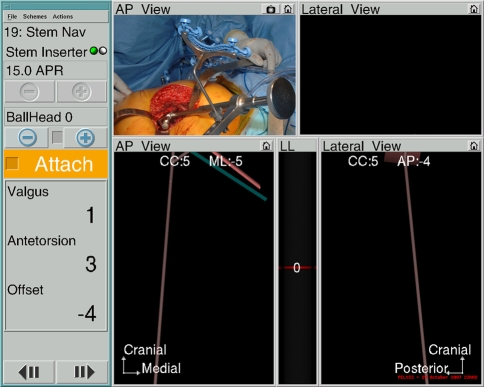
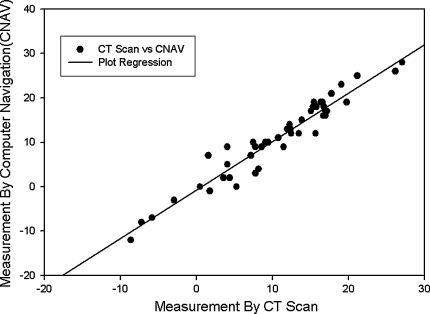
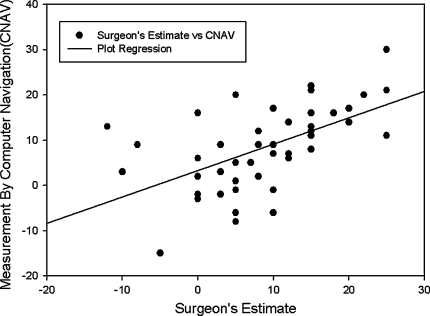
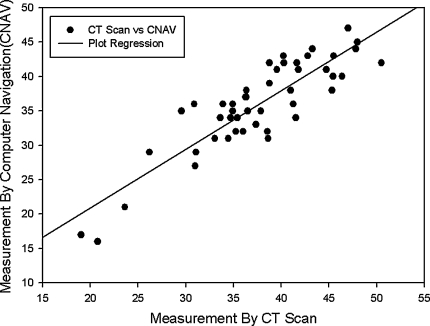
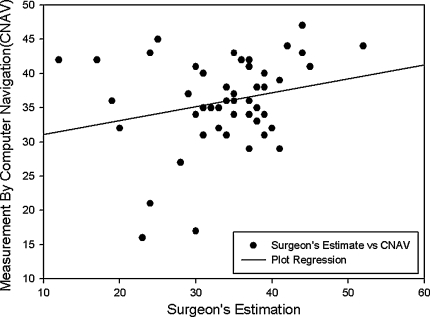
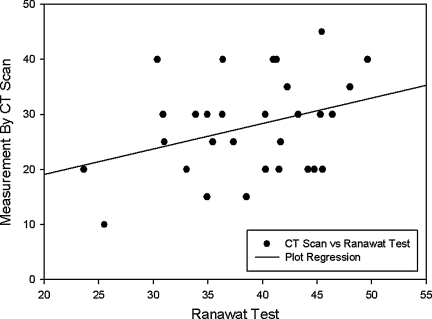
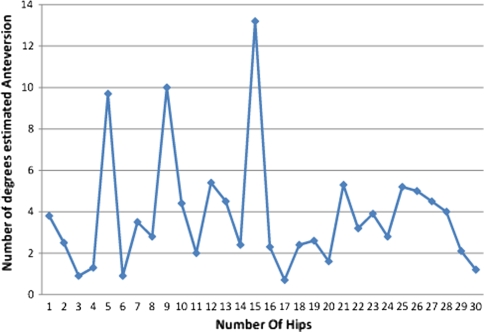
Combined cup and stem anteversion in THA based on femoral anteversion has been suggested as a method to compensate for abnormal femoral anteversion. We investigated the combined anteversion technique using computer navigation. In 47 THAs, the surgeon first estimated the femoral broach anteversion and validated the position by computer navigation. The broach was then measured with navigation. The navigation screen was blocked while the surgeon estimated the anteversion of the broach. This provided two estimates of stem anteversion. The navigated stem anteversion was validated by postoperative CT scans. All cups were implanted using navigation alone. We determined precision (the reproducibility) and bias (how close the average test number is to the true value) of the stem position. Comparing the surgeon estimate to navigation anteversion, the precision of the surgeon was 16.8 degrees and bias was 0.2 degrees ; comparing the navigation of the stem to postoperative CT anteversion, the precision was 4.8 degrees and bias was 0.2 degrees , meaning navigation is accurate. Combined anteversion by postoperative CT scan was 37.6 degrees +/- 7 degrees (standard deviation) (range, 19 degrees -50 degrees ). The combined anteversion with computer navigation was within the safe zone of 25 degrees to 50 degrees for 45 of 47 (96%) hips. Femoral stem anteversion had a wide variability.
Level of evidence: Level II, therapeutic study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures
Comment in
-
Visual intraoperative estimation of cup and stem position is not reliable in minimally invasive hip arthroplasty.Acta Orthop. 2016 Jun;87(3):225-30. doi: 10.3109/17453674.2015.1137182. Epub 2016 Feb 5. Acta Orthop. 2016. PMID: 26848628 Free PMC article.
References
-
- ASTM. Standard Practice for Use of the Terms Precision and Bias in ASTM Test Methods. In: Annual Book of ASTM Standards ed. Philadelphia, PA: American Society for Testing and Materials; 2002:E177–E190a.
-
- Bidgood WD Jr, Horii SC. Introduction to the ACR-NEMA DICOM standard. Radiographics. 1992;12:345–355. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
