

Effects of erlotinib in EGFR mutated non-small cell lung cancers with resistance to gefitinib
- PMID: 18981003
- PMCID: PMC2596582
- DOI: 10.1158/1078-0432.CCR-08-1455
Effects of erlotinib in EGFR mutated non-small cell lung cancers with resistance to gefitinib
Abstract
Purpose: Most lung cancers with activating epidermal growth factor receptor (EGFR) mutations respond to gefitinib; however, resistance to this tyrosine kinase inhibitor (TKI) invariably ensues. The T790M mutation occurs in 50% and MET amplification in 20% of TKI-resistant tumors. Other secondary mutations (D761Y and L747S) are rare. Our goal was to determine the effects of erlotinib 150 mg/d in EGFR mutated patients resistant to gefitinib 250 mg/d, because the EGFR TKI erlotinib is given at a higher biologically active dose than gefitinib.
Experimental design: Retrospective review of 18 EGFR mutated (exon 19 deletions, L858R, and L861Q) patients that were given gefitinib and subsequently erlotinib. Seven patients had tumor resampling after TKI therapy and were analyzed for secondary EGFR mutations and MET amplification.
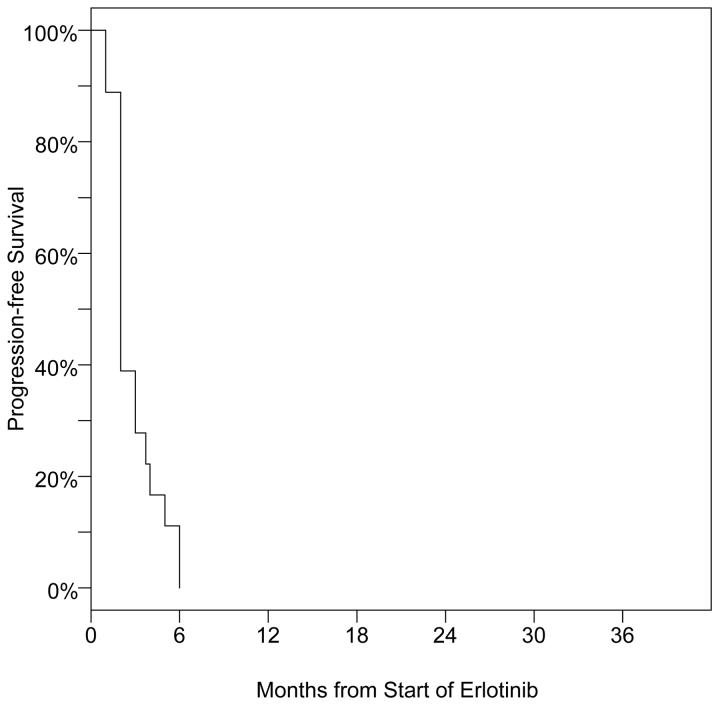
Results: Most patients (14 of 18) responded to gefitinib with median progression-free survival of 11 months (95% confidence interval, 4-16). After gefitinib resistance (de novo or acquired), 78% (14 of 18) of these patients displayed progressive disease while on erlotinib with progression-free survival of 2 months (95% confidence interval, 2-3). Six of 7 resampled patients acquired the T790M mutation, and 0 of 3 had MET amplification. Only 1 gefitinib-resistant patient with the acquired L858R-L747S EGFR, which in vitro is sensitive to achievable serum concentrations of erlotinib 150 mg/d, achieved a partial response to erlotinib.
Conclusions: In EGFR mutated tumors resistant to gefitinib 250 mg/d, a switch to erlotinib 150 mg/d does not lead to responses in most patients. These findings are consistent with preclinical models, because the common mechanisms of TKI resistance (T790M and MET amplification) in vitro are not inhibited by clinically achievable doses of gefitinib or erlotinib. Alternative strategies to overcome TKI resistance must be evaluated.
Figures

Similar articles
-
Erlotinib at a dose of 25 mg daily for non-small cell lung cancers with EGFR mutations.J Thorac Oncol. 2010 Jul;5(7):1048-53. doi: 10.1097/JTO.0b013e3181dd1386. J Thorac Oncol. 2010. PMID: 20512075 Free PMC article.
-
Acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors in non-small-cell lung cancers dependent on the epidermal growth factor receptor pathway.Clin Lung Cancer. 2009 Jul;10(4):281-9. doi: 10.3816/CLC.2009.n.039. Clin Lung Cancer. 2009. PMID: 19632948 Free PMC article. Review.
-
Clinicopathologic and molecular features of epidermal growth factor receptor T790M mutation and c-MET amplification in tyrosine kinase inhibitor-resistant Chinese non-small cell lung cancer.Pathol Oncol Res. 2009 Dec;15(4):651-8. doi: 10.1007/s12253-009-9167-8. Epub 2009 Apr 21. Pathol Oncol Res. 2009. PMID: 19381876
-
BIM mediates EGFR tyrosine kinase inhibitor-induced apoptosis in lung cancers with oncogenic EGFR mutations.PLoS Med. 2007 Oct;4(10):1669-79; discussion 1680. doi: 10.1371/journal.pmed.0040315. PLoS Med. 2007. PMID: 17973572 Free PMC article.
-
First-line treatment of advanced epidermal growth factor receptor (EGFR) mutation positive non-squamous non-small cell lung cancer.Cochrane Database Syst Rev. 2021 Mar 18;3(3):CD010383. doi: 10.1002/14651858.CD010383.pub3. Cochrane Database Syst Rev. 2021. PMID: 33734432 Free PMC article.
Cited by
-
Efficacy and safety of afatinib in Chinese patients with EGFR-mutated metastatic non-small-cell lung cancer (NSCLC) previously responsive to first-generation tyrosine-kinase inhibitors (TKI) and chemotherapy: comparison with historical cohort using erlotinib.BMC Cancer. 2016 Feb 24;16:147. doi: 10.1186/s12885-016-2201-9. BMC Cancer. 2016. PMID: 26911310 Free PMC article. Clinical Trial.
-
Crizotinib (PF-02341066) reverses multidrug resistance in cancer cells by inhibiting the function of P-glycoprotein.Br J Pharmacol. 2012 Jul;166(5):1669-83. doi: 10.1111/j.1476-5381.2012.01849.x. Br J Pharmacol. 2012. PMID: 22233293 Free PMC article.
-
Concurrent proton-pump inhibitors increase risk of death for lung cancer patients receiving 1st-line gefitinib treatment - a nationwide population-based study.Cancer Manag Res. 2019 Sep 19;11:8539-8546. doi: 10.2147/CMAR.S222278. eCollection 2019. Cancer Manag Res. 2019. PMID: 31572008 Free PMC article.
-
Erlotinib at a dose of 25 mg daily for non-small cell lung cancers with EGFR mutations.J Thorac Oncol. 2010 Jul;5(7):1048-53. doi: 10.1097/JTO.0b013e3181dd1386. J Thorac Oncol. 2010. PMID: 20512075 Free PMC article.
-
Treating ALK-positive lung cancer--early successes and future challenges.Nat Rev Clin Oncol. 2012 Apr 3;9(5):268-77. doi: 10.1038/nrclinonc.2012.43. Nat Rev Clin Oncol. 2012. PMID: 22473102 Free PMC article. Review.
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Ardizzoni A, Boni L, Tiseo M, et al. Cisplatin- versus carboplatin-based chemotherapy in first-line treatment of advanced non-small-cell lung cancer: an individual patient data meta-analysis. J Natl Cancer Inst. 2007;99:847–57. - PubMed
-
- Schiller JH, Harrington D, Belani CP, et al. Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med. 2002;346:92–8. - PubMed
-
- Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. N Engl J Med. 2006;355:2542–50. - PubMed
-
- Shepherd FA, Dancey J, Ramlau R, et al. Prospective randomized trial of docetaxel versus best supportive care in patients with non-small-cell lung cancer previously treated with platinum-based chemotherapy. J Clin Oncol. 2000;18:2095–103. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
