

Oral human papillomavirus infection before and after treatment for human papillomavirus 16-positive and human papillomavirus 16-negative head and neck squamous cell carcinoma
- PMID: 18981014
- PMCID: PMC2598779
- DOI: 10.1158/1078-0432.CCR-08-0498
Oral human papillomavirus infection before and after treatment for human papillomavirus 16-positive and human papillomavirus 16-negative head and neck squamous cell carcinoma
Abstract
Purpose: Oral human papillomavirus (HPV) infection is a risk factor for head and neck squamous cell carcinoma (HNSCC), and is a concern for patients with HPV-positive HNSCC and their partners. The prevalence of oral HPV infection before and after cancer therapy was investigated among patients with HPV16-positive and HPV16-negative HNSCC.
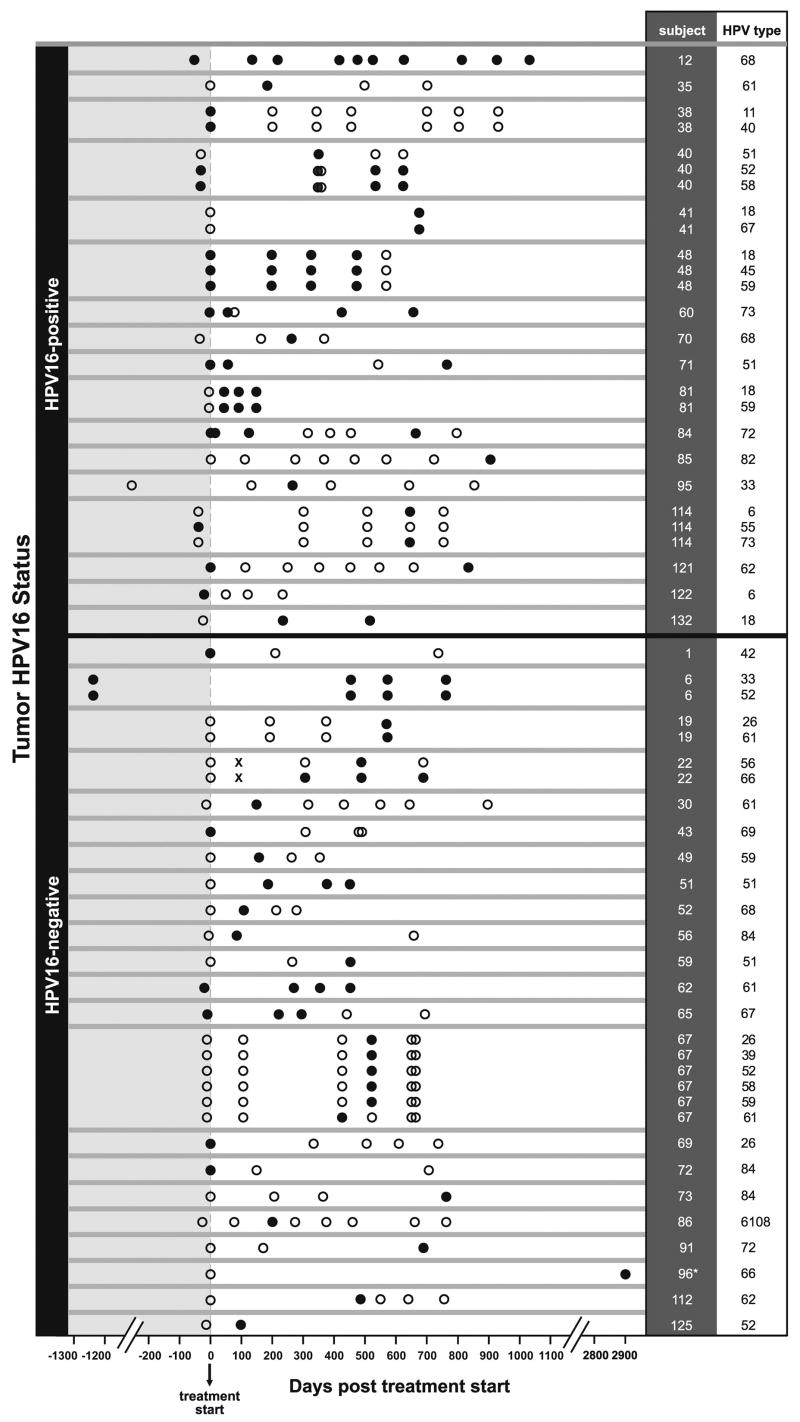
Experimental design: Serial oral rinse samples (ORS) were collected from a cohort of 135 HNSCC cases as frequently as every 3 months for up to 3 years. Tumor HPV status was determined by HPV16 in situ hybridization. HPV was detected in ORS by consensus PCR and line blot hybridization. The HPV16 variants in positive oral rinse-tumor pairs were determined by sequencing. The odds of oral HPV infection among HPV16-positive and HPV16-negative cases were compared by use of generalized estimating equations.
Results: Patients were followed for a median of 21 months and provided a median of 4 samples. Forty-four of 135 patients had HPV16-positive tumors. HPV16-positive cases were more likely than HPV16-negative cases to have an oral HPV infection detected before (odds ratio, 8.6; 95% confidence interval, 3.5-21) and after therapy (OR, 2.9; 95% confidence interval, 1.1-7.4). Oral infections by HPV16 and other high-risk, but not low-risk, types were more common among HPV16-positive cases both before and after therapy. Most HPV16 variants in ORS were European, unique, and identical to that in the tumor. Persistence of a type-specific oral infection was demonstrable for as long as 5 years.
Conclusion: Oral high-risk HPV infections are more frequent among patients with HPV16-positive than HPV16-negative HNSCC, consistent with a behavioral and/or biological disposition to infection.
Figures
Comment in
-
Genetic screening for oral human papillomavirus infections and cancers of the head and neck.Clin Cancer Res. 2008 Nov 1;14(21):6723-4. doi: 10.1158/1078-0432.CCR-08-1915. Clin Cancer Res. 2008. PMID: 18980962
References
-
- Hansson BG, Rosenquist K, Antonsson A, et al. Strong association between infection with human papillomavirus and oral and oropharyngeal squamous cell carcinoma: a population-based case-control study in southern Sweden. Acta Otolaryngol. 2005;125:1337–44. - PubMed
-
- Pintos J, Black MJ, Sadeghi N, et al. Human papillomavirus infection and oral cancer: a case-control study in Montreal, Canada. Oral Oncol. 2008;44:242–50. - PubMed
-
- Smith EM, Ritchie JM, Summersgill KF, et al. Human papillomavirus in oral exfoliated cells and risk of head and neck cancer. J Natl Cancer Inst. 2004;96:449–55. - PubMed
-
- D’Souza G, Kreimer AR, Viscidi R, et al. Case-control study of human papillomavirus and oropharyngeal cancer. N Engl J Med. 2007;356:1944–56. - PubMed
-
- Mork J, Lie AK, Glattre E, et al. Human papillomavirus infection as a risk factor for squamous-cell carcinoma of the head and neck. N Engl J Med. 2001;344:1125–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
