

A kinematic and electromyographic analysis of turning in people with Parkinson disease
- PMID: 18981189
- PMCID: PMC2649739
- DOI: 10.1177/1545968308320639
A kinematic and electromyographic analysis of turning in people with Parkinson disease
Abstract
Background: Parkinson disease frequently causes difficulty turning that can lead to falls, loss of independence, and diminished quality of life. Turning in tight spaces, which may be particularly impaired in Parkinson disease, is an essential part of our daily lives, yet a comprehensive analysis of in-place turning has not been published.
Objective: This study was conducted to determine whether there are objective differences in turning between people with Parkinson disease and unimpaired people.
Methods: In-place turning with kinematics and electromyographic measures was characterized in 11 participants with Parkinson disease and 12 healthy people. Kinematic data were recorded using a 3-dimensional motion capture system in synchrony with electromyographic data from lower extremity muscles as participants turned 180 degrees . Those with Parkinson disease were tested after overnight withdrawal of medication.
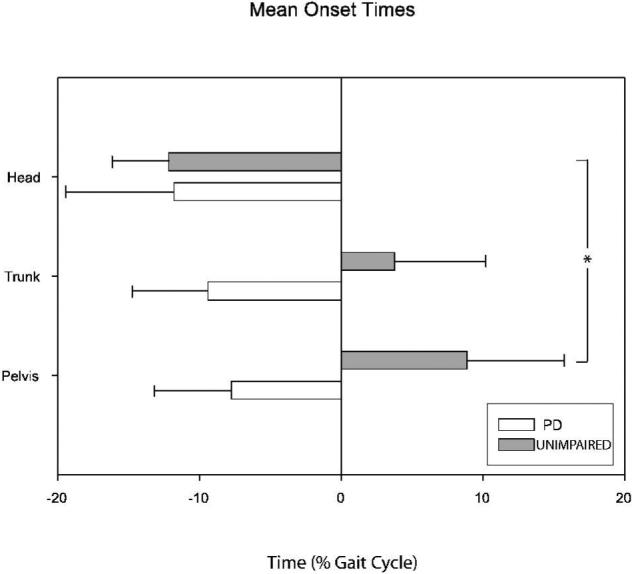
Results: Both groups used 2 distinct turning strategies. In one, the foot ipsilateral to the turning direction initiated the turn; in the other, the foot contralateral to the turning direction initiated the turn. Kinematic analysis demonstrated a craniocaudal sequence of turning in the unimpaired group, whereas those with Parkinson disease had a simultaneous onset of yaw rotation of the head, trunk, and pelvis. They also took a longer time and more steps to complete turns. Overall, lower extremity muscle activation patterns appeared similar between groups.
Conclusion: Differences between the groups were noted for axial control, but lower extremity muscle patterns were similar. This work may provide the foundation for development of new treatments for turning difficulty in Parkinson disease.
Figures







References
-
- Nieuwboer A, De Weerdt W, Dom R, Lesaffre E. A frequency and correlation analysis of motor deficits in Parkinson patients. Disabil Rehabil. 1998;20(4):142–50. - PubMed
-
- Bloem BR, Grimbergen YA, Cramer M, Willemsen M, Zwinderman AH. Prospective assessment of falls in Parkinson's disease. J Neurol. 2001;248(11):950–8. - PubMed
-
- Stack EL, Ashburn AM, Jupp KE. Strategies used by people with Parkinson's disease who report difficulty turning. Parkinsonism Relat Disord. 2006;12(2):87–92. - PubMed
-
- Giladi N, McMahon D, Przedborski S. Motor blocks in Parkinson's disease. Neurology. 1992;42:333–339. - PubMed
-
- Charlett A, Weller C, Purkiss A, Dobbs S, Dobbs R. Breadth of base whilst walking: effect of ageing and parkinsonism. Age Ageing. 1998;27:48–54. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
