

Viral resuppression and detection of drug resistance following interruption of a suppressive non-nucleoside reverse transcriptase inhibitor-based regimen
- PMID: 18981767
- PMCID: PMC2745911
- DOI: 10.1097/QAD.0b013e328311d16f
Viral resuppression and detection of drug resistance following interruption of a suppressive non-nucleoside reverse transcriptase inhibitor-based regimen
Abstract
Background: Interruption of a non-nucleoside reverse transcriptase inhibitor (NNRTI)-regimen is often necessary, but must be performed with caution because NNRTIs have a low genetic barrier to resistance. Limited data exist to guide clinical practice on the best interruption strategy to use.
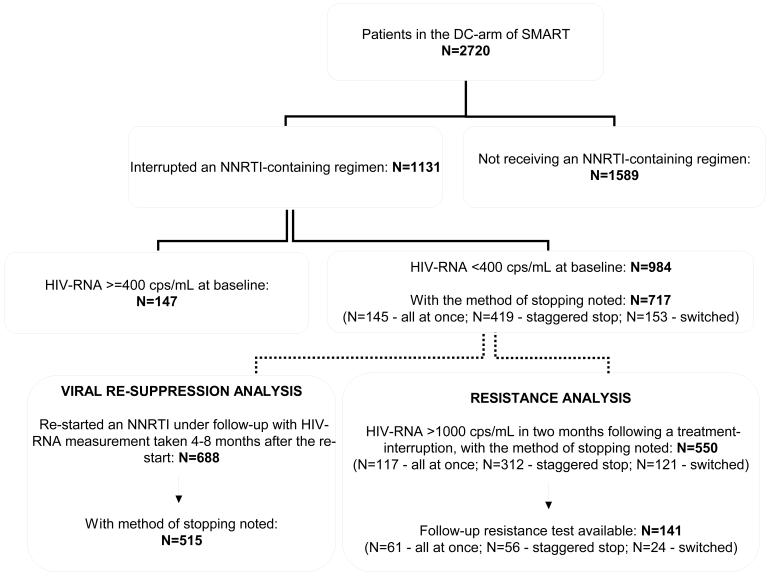
Methods: Patients in the drug-conservation arm of the Strategies for Management of Antiretroviral Therapy (SMART) trial who interrupted a fully suppressive NNRTI-regimen were evaluated. From 2003, SMART recommended interruption of an NNRTI by a staggered interruption, in which the NNRTI was stopped before the NRTIs, or by replacing the NNRTI with another drug before interruption. Simultaneous interruption of all antiretrovirals was discouraged. Resuppression rates 4-8 months after reinitiating NNRTI-therapy were assessed, as was the detection of drug-resistance mutations within 2 months of the treatment interruption in a subset (N = 141).
Results: Overall, 601/688 (87.4%) patients who restarted an NNRTI achieved viral resuppression. The adjusted odds ratio (95% confidence interval) for achieving resuppression was 1.94 (1.02-3.69) for patients with a staggered interruption and 3.64 (1.37-9.64) for those with a switched interruption compared with patients with a simultaneous interruption. At least one NNRTI-mutation was detected in the virus of 16.4% patients with simultaneous interruption, 12.5% patients with staggered interruption and 4.2% patients with switched interruption. Fewer patients with detectable mutations (i.e. 69.2%) achieved HIV-RNA of 400 copies/ml or less compared with those in whom no mutations were detected (i.e. 86.7%; P = 0.05).
Conclusion: In patients who interrupt a suppressive NNRTI-regimen, the choice of interruption strategy may influence resuppression rates when restarting a similar regimen. NNRTI drug-resistance mutations were observed in a relatively high proportion of patients. These data provide additional support for a staggered or switched interruption strategy for NNRTI drugs.
Trial registration: ClinicalTrials.gov NCT00027352.
Figures
References
-
- El-Sadr WM, Lundgren JD, Neaton JD, Gordin F, Abrams D, Arduino RC, et al. CD4+ count-guided interruption of antiretroviral treatment. New England Journal of Medicine. 2006;355(22):2283–2296. - PubMed
-
- Arduino R. CD4 cell count-guided treatment interruption: Be smart and wait for more evidence. Clinical Infectious Diseases. 2005;40(5):735–737. - PubMed
-
- Robbins BL, Srinivas RV, Kim C, Bischofberger N, Fridland A. Anti-human immunodeficiency virus activity and cellular metabolism of a potential prodrug of the acyclic nucleoside phosphonate 9-R-(2-phosphonomethoxypropyl)adenine (PMPA), Bis(isopropyloxymethylcarbonyl)PMPA. Antimicrob Agents Chemother. 1998;42(3):612–617. - PMC - PubMed
-
- Ribaudo HJ, Haas DW, Tierney C, Kim RB, Wilkinson GR, Gulick RM, et al. Pharmacogenetics of plasma efavirenz exposure after treatment discontinuation: an Adult AIDS Clinical Trials Group Study. Clin Infect Dis. 2006;42(3):401–407. - PubMed
-
- Taylor S, Boffito M, Khoo S, Smit E, Back D. Stopping antiretroviral therapy. AIDS. 2007;21(13):1673–1682. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
