

The feasibility of single port laparoscopic cholecystectomy: a pilot study of 20 cases
- PMID: 18982149
- PMCID: PMC2575680
- DOI: 10.1080/13651820802276622
The feasibility of single port laparoscopic cholecystectomy: a pilot study of 20 cases
Abstract
Introduction: Laparoscopic cholecystectomy has become the gold standard for symptomatic cholelithiasis. Traditionally done through four ports, three and two port surgeries have been described. We present a novel technique of single port cholecystectomy using the R-Port (Advanced Surgical Concepts).
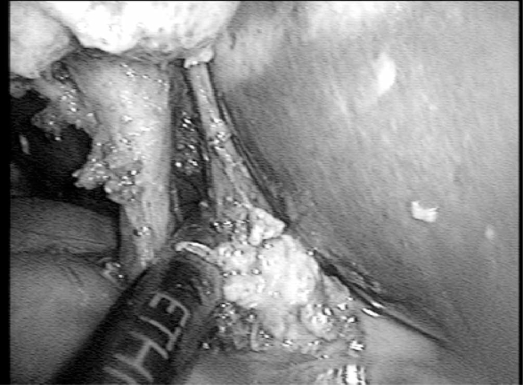
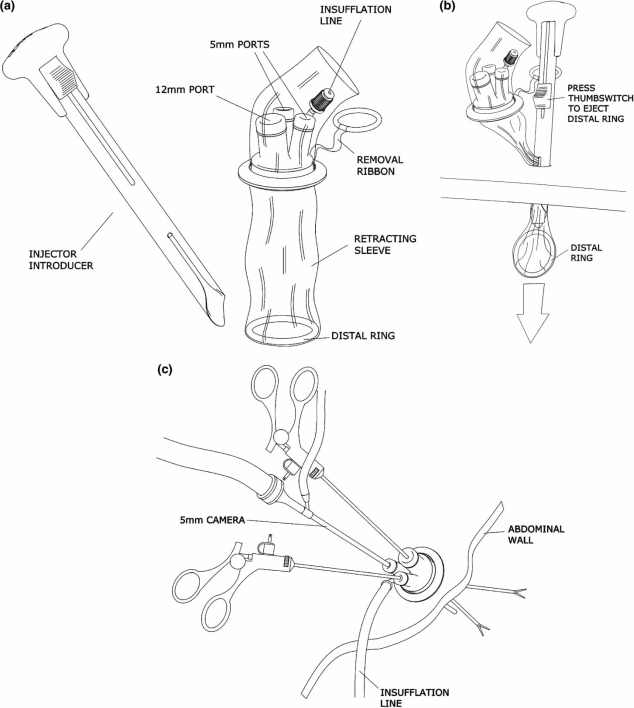
Materials and methods: The R-Port is a Tri-port that allows the ingress of three 5 mm instruments through a single port. Twenty patients with symptomatic cholelithiasis were subjected to single port cholecystectomy using the R-Port through the umbilicus. Two patients also had choledocholithiasis. Modified instruments with angulated shafts were used for the surgery. A telescope with a coaxial light cable was also used. Whenever necessary, an extra needle for retraction or an additional 5 mm port was used.
Results: Single port laparoscopic was accomplished in 17 of the 20 patients. In one patient an additional port was used for the cholecystectomy and in two others it was used for the common bile duct exploration but not for the dissection of Calot's triangle. Of the 17 patients, seven needed a single needle to retract the fundus of the gall bladder.
Conclusions: Single port laparoscopic cholecystectomy is feasible and safe using the R-Port. The level of difficulty is higher and a needle for retraction or an additional port may be used whenever the visualization of Calot's triangle is unsatisfactory. Further studies and the development of better instrumentation are necessary before this can be recommended as a standard procedure.
Keywords: cholecystectomy; laparoscopy; single port.
Figures





References
-
- Begos DG, Modlin IM. LC: from gimmick to gold standard. J Clin Gast. 1994;19(4):325–30. - PubMed
-
- Cuschieri A, Dubois F, Mouiel J, Mouret P, Becker H, Buess G, et al. The European experience with laparoscopic cholecystectomy. Ann J Surg. 1991;161:385–7. - PubMed
-
- Giacomo U, Alfonso MM, Gioacchino C, Gaspere G, David B, Arianna CS. Laparoscopic cholecystectomy: European position versus American position. Revista de Ciência de Saúde de Macau. 2002;2(1 & 2):32–4.
-
- Kagaya T. Laparoscopic cholecystectomy via two ports, using the “Twin-Port” system. J Hepatobiliary Pancreat Surg. 2001;8(1):76–80. - PubMed
-
- Trichak S. 3 port v/s 4 port cholecystectomy. Surg Endosc. 2003;17(9):1434–36. - PubMed
LinkOut - more resources
Full Text Sources
Medical
