

Cognitive expertise, emotional development, and reflective capacity: clinical skills for improved pain care
- PMID: 18984501
- PMCID: PMC2596981
- DOI: 10.1016/j.jpain.2008.07.010
Cognitive expertise, emotional development, and reflective capacity: clinical skills for improved pain care
Abstract
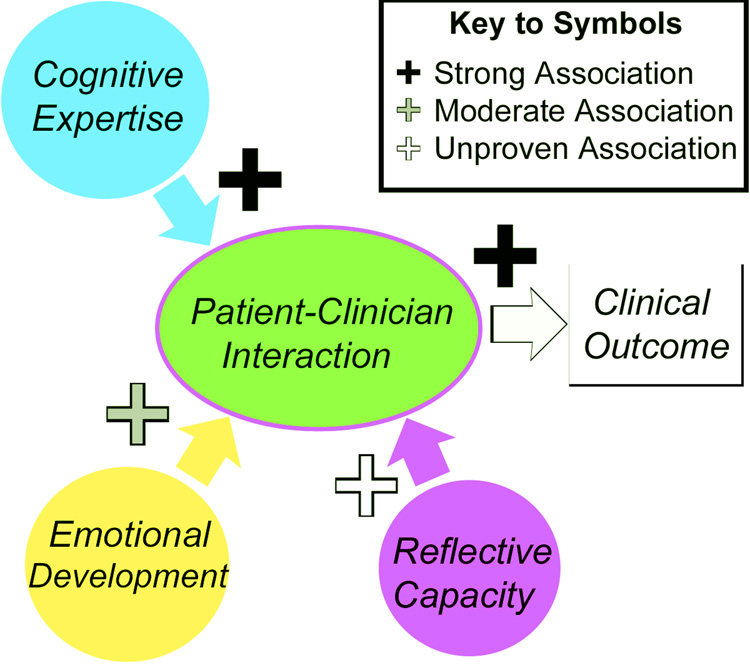
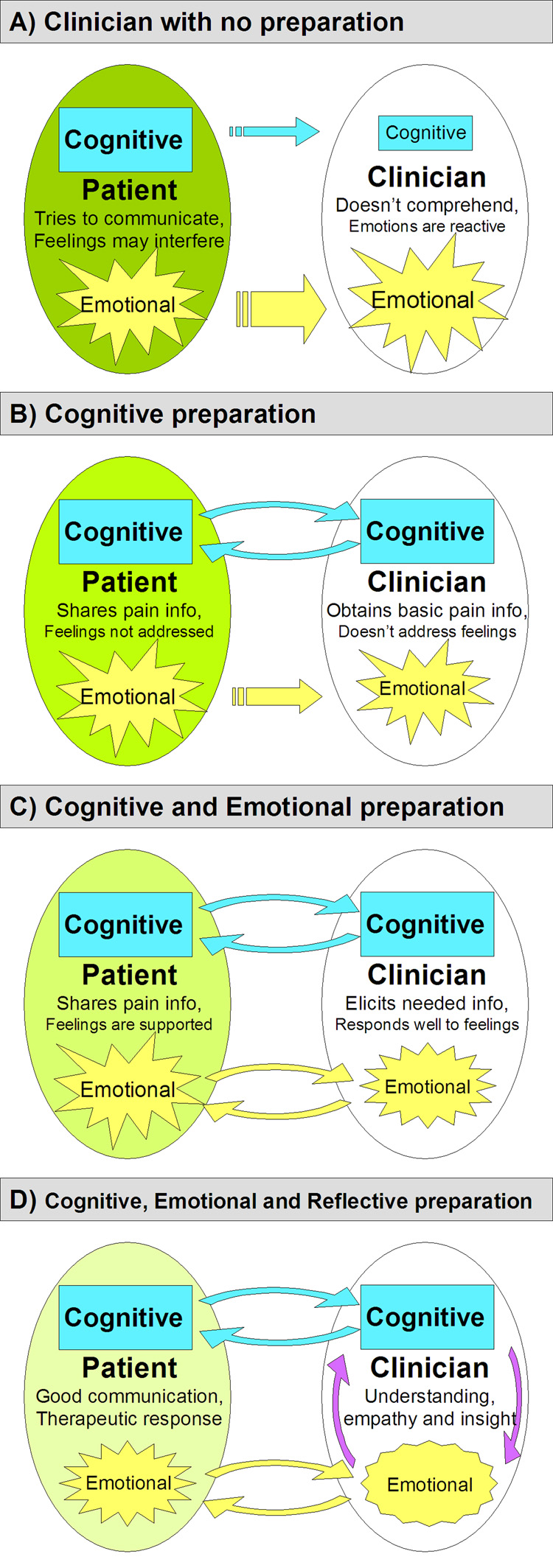
The overarching goal of medical training is to nurture the growth of knowledgeable, caring, and insightful clinicians guided by the ideals of medical professionalism. Recent definitions of professional competence identify essential clinical skills, including cognitive expertise, emotional competence, and reflective capacity. This modern framework reflects the increasingly complex nature of the patient-clinician interaction, in which the clinician must exchange diagnostic information while supportively engaging the patient on a deeper, affective level. The affective dimension can be particularly potent when pain is the primary symptom, as it is for the majority of medical visits. Unfortunately, however, current models of professionalism, used as an early guide for medical trainees to develop an understanding of the clinical exchange, largely focus on interactions in the cognitive domain. To emphasize the importance of emotions in professional development, we propose the Cognitive and Emotional Preparedness Model, which describes the clinical encounter occurring on two channels, one cognitive and the other emotional, and stresses the importance of multidimensional development in preparing the clinician to (1) communicate clinical information, (2) provide emotional support, and (3) actively reflect on experiences for continued improvement. Together, acquisition of knowledge, emotional development, and reflective skill will improve the clinical interaction.
Perspective: The proficiency of medical trainees in developing clinical skills profoundly shapes patient satisfaction and treatment outcomes. This article reviews the cognitive, emotional, and reflective development of medical trainees and presents a model illustrating how clinical development impacts pain care. For improved efficacy, pain education should be calibrated to students' developmental needs.
Figures
Similar articles
-
Student and educator experiences of maternal-child simulation-based learning: a systematic review of qualitative evidence protocol.JBI Database System Rev Implement Rep. 2015 Jan;13(1):14-26. doi: 10.11124/jbisrir-2015-1694. JBI Database System Rev Implement Rep. 2015. PMID: 26447004
-
Reflective practice and its role in facilitating creative responses to dilemmas within clinical communication - a qualitative analysis.BMC Med Educ. 2016 Nov 24;16(1):301. doi: 10.1186/s12909-016-0823-x. BMC Med Educ. 2016. PMID: 27881123 Free PMC article.
-
Adapting to the emotional complexity of palliative care communication: Palliative care clinicians' experiences.Palliat Support Care. 2025 Jan 21;23:e43. doi: 10.1017/S1478951524001883. Palliat Support Care. 2025. PMID: 39834275
-
Integrating cognitive and affective dimensions of pain experience into health professions education.Pain Res Manag. 2011 Nov-Dec;16(6):421-6. doi: 10.1155/2011/424978. Pain Res Manag. 2011. PMID: 22184551 Free PMC article. Review.
-
Defining and assessing professional competence.JAMA. 2002 Jan 9;287(2):226-35. doi: 10.1001/jama.287.2.226. JAMA. 2002. PMID: 11779266 Review.
Cited by
-
Systematic Review of Pain Medicine Content, Teaching, and Assessment in Medical School Curricula Internationally.Pain Ther. 2018 Dec;7(2):139-161. doi: 10.1007/s40122-018-0103-z. Epub 2018 Jul 30. Pain Ther. 2018. PMID: 30058045 Free PMC article. Review.
-
The Pain Medicine Curriculum Framework-structured integration of pain medicine education into the medical curriculum.Front Pain Res (Lausanne). 2023 Jan 9;3:1057114. doi: 10.3389/fpain.2022.1057114. eCollection 2022. Front Pain Res (Lausanne). 2023. PMID: 36700142 Free PMC article. Review.
-
Pain, comorbidities, and clinical decision-making: conceptualization, development, and pilot testing of the Pain in Aging, Educational Assessment of Need instrument.Front Pain Res (Lausanne). 2024 Feb 22;5:1254792. doi: 10.3389/fpain.2024.1254792. eCollection 2024. Front Pain Res (Lausanne). 2024. PMID: 38455875 Free PMC article.
-
Domains of Students' Concerns in Oral Diagnosis and Surgery Clinic.Clin Cosmet Investig Dent. 2023 Aug 21;15:157-163. doi: 10.2147/CCIDE.S425318. eCollection 2023. Clin Cosmet Investig Dent. 2023. PMID: 37637075 Free PMC article.
-
The effects of educational interventions on pharmacists' knowledge, attitudes and beliefs towards low back pain.Int J Clin Pharm. 2015 Aug;37(4):616-25. doi: 10.1007/s11096-015-0112-5. Epub 2015 Apr 8. Int J Clin Pharm. 2015. PMID: 25851502
References
-
- Bellini LM, Shea JA. Mood change and empathy decline persist during three years of internal medicine training. Acad Med. 2005;80:164–167. - PubMed
-
- Blasco PG, Moreto G, Levites M. Teaching humanities through opera: leading medical students to reflective attitudes. Fam Med. 2005;37:18–20. - PubMed
-
- Bowman D, Hughes P. Emotional responses of tutors and students in problem-based learning: lessons for staff development. Med Educ. 2005;39:145–153. - PubMed
-
- Bradley JG, Zia MJ, Hamilton N. Patient preferences for control in medical decision making: a scenario-based approach. Fam Med. 1996;28:496–501. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
