

Transmural recording of shock potential gradient fields, early postshock activations, and refibrillation episodes associated with external defibrillation of long-duration ventricular fibrillation in swine
- PMID: 18984539
- PMCID: PMC2628804
- DOI: 10.1016/j.hrthm.2008.08.019
Transmural recording of shock potential gradient fields, early postshock activations, and refibrillation episodes associated with external defibrillation of long-duration ventricular fibrillation in swine
Abstract
Background: Knowledge of the shock potential gradient (nablaV) and postshock activation is limited to internal defibrillation of short-duration ventricular fibrillation (SDVF).
Objective: The purpose of this study was to determine these variables after external defibrillation of long-duration VF (LDVF).
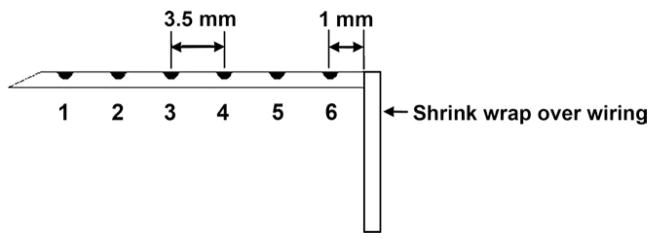
Methods: In six pigs, 115-20 plunge needles with three to six electrodes each were inserted to record throughout both ventricles. After the chest was closed, the biphasic defibrillation threshold (DFT) was determined after 20 seconds of SDVF with external defibrillation pads. After 7 minutes of LDVF, defibrillation shocks that were less than or equal to the SDVF DFT strength were given.
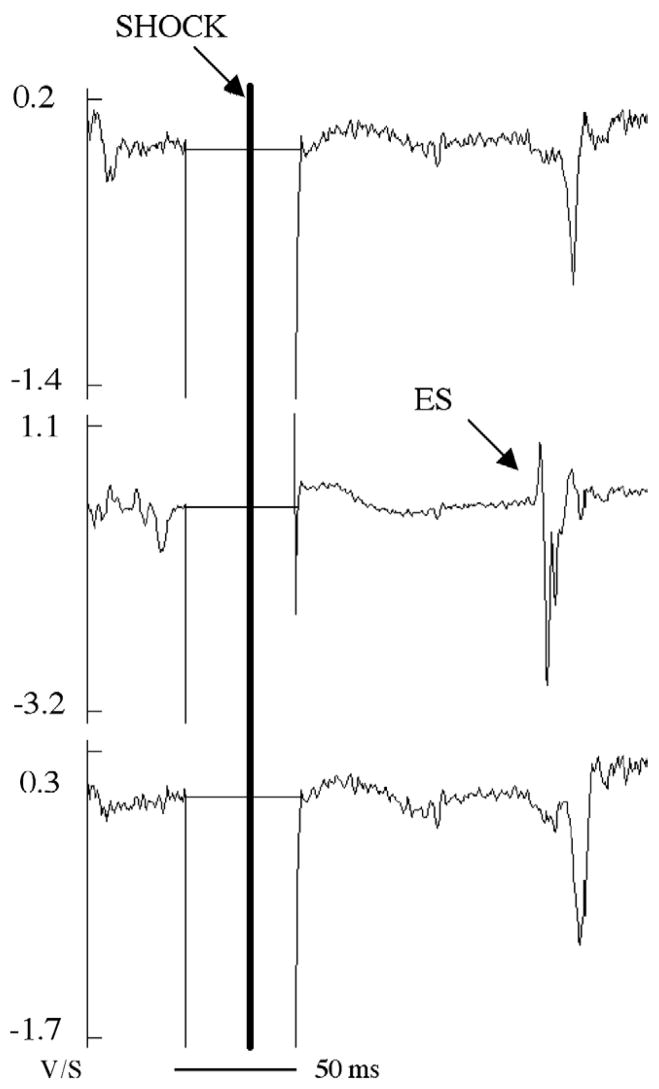
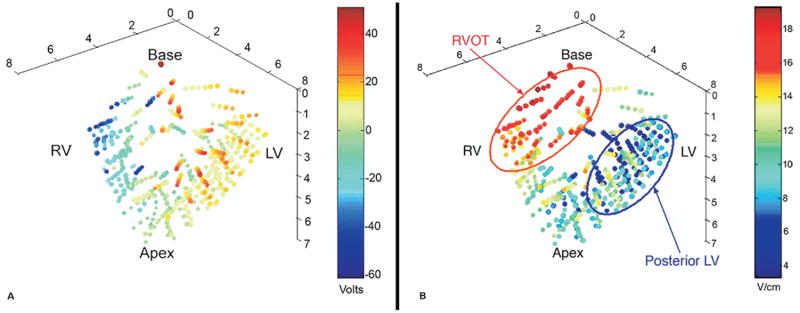
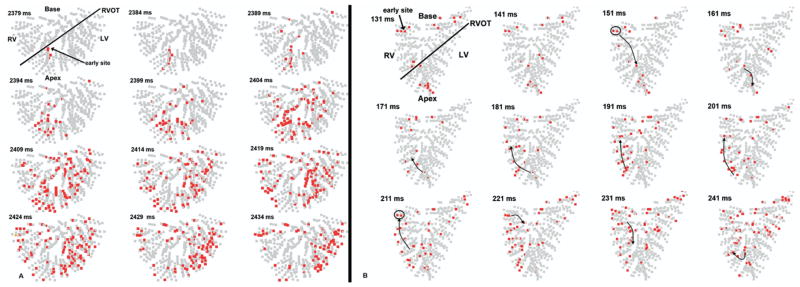
Results: For DFT shocks (1632 +/- 429 V), the maximum minus minimum ventricular voltage (160 +/- 100 V) was 9.8% of the shock voltage. Maximum cardiac nablaV (28.7 +/- 17 V/cm) was 4.7 +/- 2.0 times the minimum nablaV (6.2 +/- 3.5 V/cm). Although LDVF did not increase the DFT in five of the six pigs, it significantly lengthened the time to earliest postshock activation following defibrillation (1.6 +/- 2.2 seconds for SDVF and 4.9 +/- 4.3 seconds for LDVF). After LDVF, 1.3 +/- 0.8 episodes of spontaneous refibrillation occurred per animal, but there was no refibrillation after SDVF.
Conclusion: Compared with previous studies of internal defibrillation, during external defibrillation much less of the shock voltage appears across the heart and the shock field is much more even; however, the minimum nablaV is similar. Compared with external defibrillation of SDVF, the biphasic external DFT for LDVF is not increased; however, time to earliest postshock activation triples. Refibrillation is common after LDVF but not after SDVF in these normal hearts, indicating that LDVF by itself can cause refibrillation without requiring preexisting heart disease.
Figures

Comment in
-
Long versus short duration fibrillation: what's the difference?Heart Rhythm. 2008 Nov;5(11):1607-8. doi: 10.1016/j.hrthm.2008.08.025. Epub 2008 Aug 28. Heart Rhythm. 2008. PMID: 18984540 No abstract available.
References
-
- Cobb LA, Fahrenbruch CE, Walsh TR, et al. Influence of cardiopulmonary resuscitation prior to defibrillation in patients with out-of-hospital ventricular fibrillation. JAMA. 1999;281:1182–1188. - PubMed
-
- Wiggers CJ. The mechanism and nature of ventricular fibrillation. Am Heart J. 1940;20:399–412.
-
- Allison JS, Qin H, Dosdall DJ, et al. The transmural activation sequence in porcine and canine left ventricle is markedly different during long-duration ventricular fibrillation. J Cardiovasc Electrophysiol. 2007;18:1306–1312. - PubMed
-
- Garcia LA, Allan JJ, Kerber RE. Interactions between CPR and defibrillation waveforms: effect on resumption of a perfusing rhythm after defibrillation. Resuscitation. 2000;47:301–305. - PubMed
-
- White RD, Russell JK. Refibrillation, resuscitation and survival in out-of-hospital sudden cardiac arrest victims treated with biphasic automated external defibrillators. Resuscitation. 2002;55:17–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
