

Metabolic and hormonal changes induced by pioglitazone in polycystic ovary syndrome: a randomized, placebo-controlled clinical trial
- PMID: 18984667
- PMCID: PMC2646515
- DOI: 10.1210/jc.2008-1133
Metabolic and hormonal changes induced by pioglitazone in polycystic ovary syndrome: a randomized, placebo-controlled clinical trial
Abstract
Context: Polycystic ovary syndrome (PCOS) is characterized by insulin resistance, compensatory hyperinsulinemia, increased prevalence of impaired glucose tolerance, and increased ovarian androgen biosynthesis.
Objective: The aim of the study was to evaluate effects of pioglitazone on whole body insulin action and ovarian androgen biosynthesis in PCOS.
Design: We performed a randomized placebo-controlled trial.
Setting: The study was conducted at the Special Diagnostic and Treatment Unit of the Veterans Affairs Medical Center, San Diego, and the University of California, San Diego, General Clinical Research Center.
Patients or other participants: A total of 23 subjects with PCOS were evaluated at baseline and end of treatment. Six age- and body mass index-matched women without PCOS were normal controls for baseline evaluation.
Intervention: Subjects with PCOS were randomized to oral placebo or pioglitazone 45 mg daily for 6 months.
Main outcome measure(s): The primary outcome measures were whole body insulin action as measured by hyperinsulinemic euglycemic clamp and ovarian androgen biosynthesis as measured by leuprolide-stimulated production of 17-hydroxyprogesterone (17-OHP).
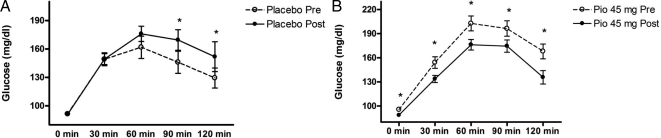
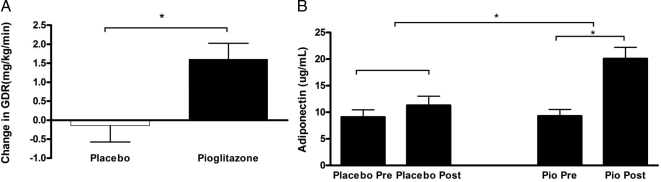
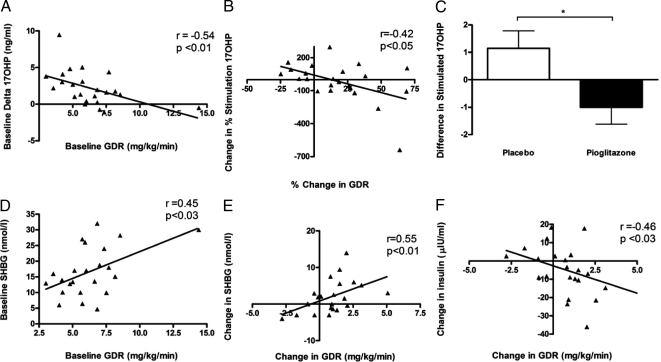
Results: Compared with placebo, pioglitazone treatment significantly improved multiple measures of insulin action, including glucose disposal rate (P < 0.01), 2-h glucose during 75-g oral glucose tolerance test (P < 0.01), area under the curve glucose during oral glucose tolerance test (P < 0.01), serum adiponectin (P < 0.01), and fasting hyperinsulinemia (P < 0.01). Compared to placebo, pioglitazone treatment reduced the increment of leuprolide-stimulated 17-OHP (P < 0.02). Improvements in glucose disposal rate correlated with reductions in 17-OHP stimulation (P < 0.02).
Conclusions: Compared to placebo, pioglitazone treatment in PCOS was associated with improvements in insulin action and glucose homeostasis and ameliorated the hyperandrogenic ovarian response.
Figures
References
-
- Azziz R, Woods KS, Reyna R, Key TJ, Knochenhauer ES, Yildiz BO 2004 The prevalence and features of the polycystic ovary syndrome in an unselected population. J Clin Endocrinol Metab 89:2745–2749 - PubMed
-
- Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, Azziz R 1998 Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: a prospective study. J Clin Endocrinol Metab 83:3078–3082 - PubMed
-
- Legro RS, Kunselman AR, Dodson WC, Dunaif A 1999 Prevalence and predictors of risk for type 2 diabetes mellitus and impaired glucose tolerance in polycystic ovary syndrome: a prospective, controlled study in 254 affected women. J Clin Endocrinol Metab 84:165–169 - PubMed
-
- Dunaif A, Segal KR, Futterweit W, Dobrjansky A 1989 Profound peripheral insulin resistance, independent of obesity, in polycystic ovary syndrome. Diabetes 38:1165–1174 - PubMed
-
- Ek I, Arner P, Bergqvist A, Carlström K, Wahrenberg H 1997 Impaired adipocyte lipolysis in nonobese women with the polycystic ovary syndrome: a possible link to insulin resistance? J Clin Endocrinol Metab 82:1147–1153 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
