

Improving vastus medialis obliquus function reduces pressure applied to lateral patellofemoral cartilage
- PMID: 18985700
- PMCID: PMC2669691
- DOI: 10.1002/jor.20791
Improving vastus medialis obliquus function reduces pressure applied to lateral patellofemoral cartilage
Abstract
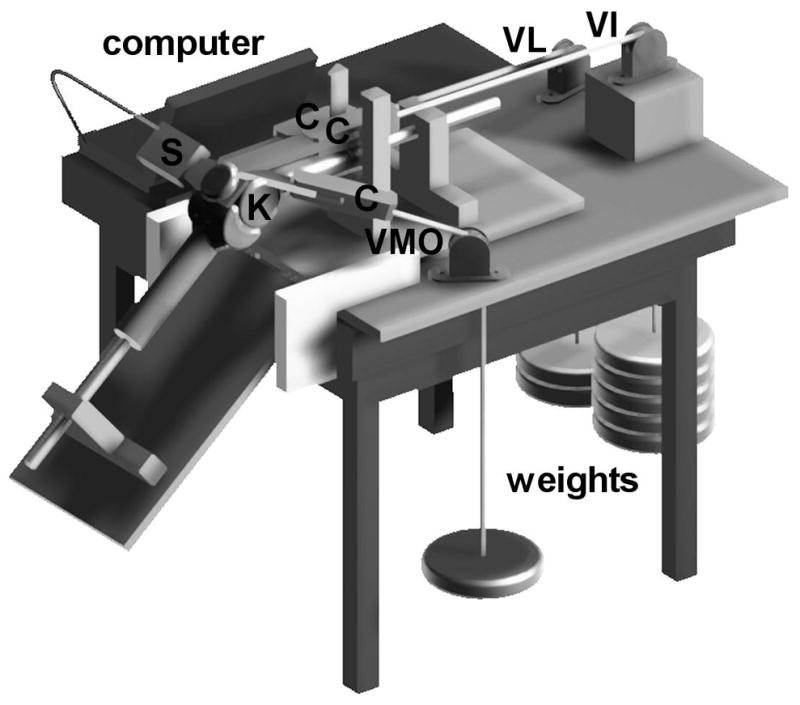
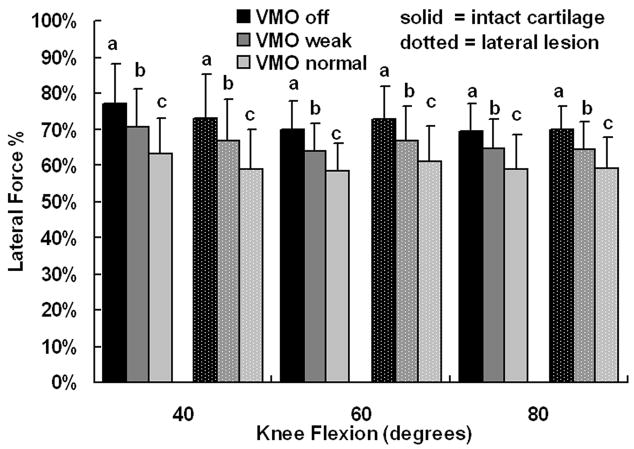
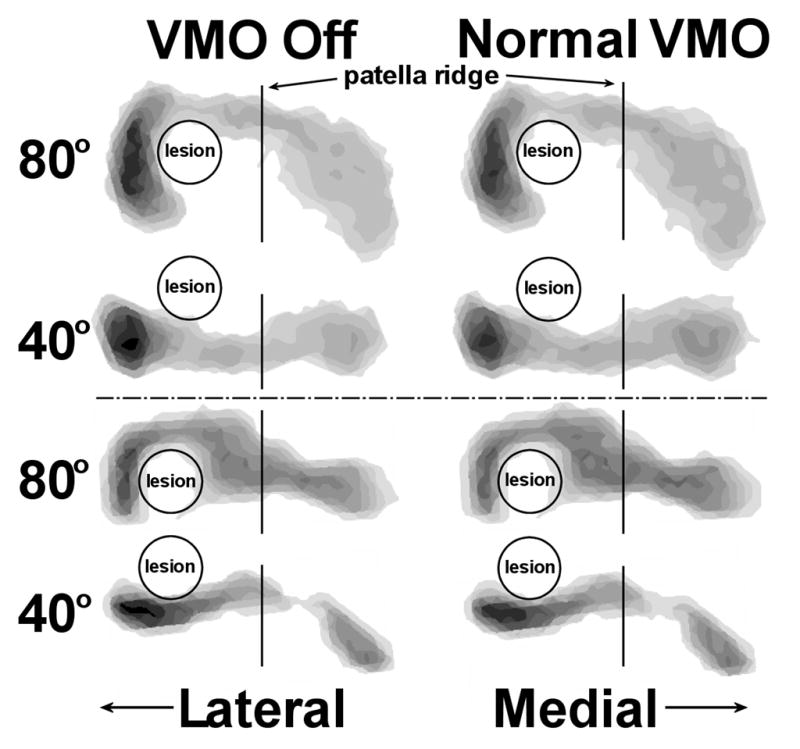
The current study was performed to characterize how improving vastus medialis obliquus (VMO) function influences the pressure applied to patellofemoral cartilage. An additional focus was characterizing how lateral and medial cartilage lesions influence cartilage pressures. Ten knees were flexed to 40 degrees, 60 degrees, and 80 degrees in vitro, and forces were applied to represent the VMO and other muscles of the quadriceps group while a thin film sensor measured joint pressures. The knees were loaded with a normal VMO force, with the VMO force decreased by approximately 50%, and with the VMO unloaded. After tests were performed with the cartilage intact, all tests were repeated with a 12-mm-diameter lesion created within the lateral cartilage, with the lateral lesion repaired with silicone, and with a medial lesion created. Based on a two-way repeated measures ANOVA and post-hoc tests, increasing the force applied by the VMO significantly (p < 0.05) decreased the maximum lateral pressure and significantly increased the maximum medial pressure at each flexion angle. A lateral cartilage lesion significantly increased the maximum lateral pressure, while a medial lesion did not significantly influence the maximum medial pressure. Improving VMO function can reduce the pressure applied to lateral cartilage when lateral lesions are present.
Copyright 2008 Orthopaedic Research Society
Figures


References
-
- Bicos J, Fulkerson JP, Amis A. Current concepts review: the medial patellofemoral ligament. Am J Sports Med. 2007;35:484–92. - PubMed
-
- Steiner TM, Torga-Spak R, Teitge RA. Medial patellofemoral ligament reconstruction in patients with lateral patellar instability and trochlear dysplasia. Am J Sports Med. 2006;34:1254–61. - PubMed
-
- Fulkerson JP, Shea KP. Disorders of patellofemoral alignment. J Bone Joint Surg Am. 1990;72:1424–1429. - PubMed
-
- Saleh KJ, Arendt EA, Eldridge J, et al. Operative Treatment of Patellofemoral Arthritis. J Bone Joint Surg Am. 2005;87:659–671. - PubMed
-
- Fulkerson JP. Diagnosis and treatment of patients with patellofemoral pain. Am J Sports Med. 2002;30:447–456. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
