

Intensive chemotherapy for systemic anaplastic large cell lymphoma in children and adolescents: final results of Children's Cancer Group Study 5941
- PMID: 18985718
- PMCID: PMC2769495
- DOI: 10.1002/pbc.21817
Intensive chemotherapy for systemic anaplastic large cell lymphoma in children and adolescents: final results of Children's Cancer Group Study 5941
Abstract
Background: Anaplastic large cell lymphoma (ALCL) is characterized by advanced disease at presentation (70-80% of pediatric cases) and accounts for 10-15% of all childhood lymphomas. Treatment strategies for pediatric ALCL vary from short pulse B-NHL chemotherapy to prolonged leukemia like therapy. The optimal treatment strategy is unknown.
Methods: CCG-5941 used a compressed aggressive multiagent T-cell lineage chemotherapy regimen consisting of a 3-week induction therapy (vincristine, prednisone, cyclophosphamide, daunomycin, asparaginase) followed by a 3-week consolidation period (vincristine, prednisone, etoposide, 6-thioguanine, cytarabine, asparaginase, methotrexate) followed by six courses of maintenance chemotherapy at 7-week intervals (cyclophosphamide, 6-thioguanine, vincristine, prednisone, doxorubicin, asparaginase, methotrexate etoposide, cytarabine). Total therapy was 48 weeks.
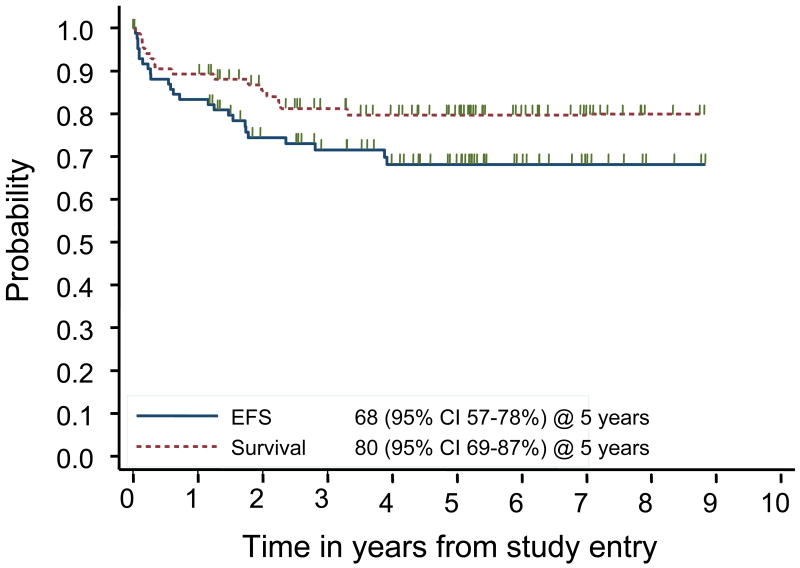
Results: Eighty-six children (male 56%, female 44%) with non-localized ALCL (CD30+) were treated. The majority of tumors were positive for ALK (90%) and of T lineage (83%). Extranodal disease was common (mediastinum 35%, skin 15%, lung 14%, bone 12%, bone marrow 13%, liver 6%, and other viscera 17%). Grade 4 neutropenia occurred in 82% of patients. The 5-year EFS was 68% (95% CI of 57-78%) and the 5-year OS was 80% (95% CI of 69-87%). There were 21 relapses and 4 toxic deaths as first events. Relapse occurred early with 17 (81%) relapses occurring within 2 years of diagnosis and 12 (57%) while receiving therapy. Univariate analysis for risk factors only identified bone marrow involvement predicting lower EFS (P = 0.03).
Conclusions: CCG-5941 demonstrated efficacy similar to previously reported regimens but with significant hematologic toxicity.
Figures
References
-
- Sandlund JT, Downing JR, Crist WM. Non-Hodgkin's lymphoma in childhood. N Engl J Med. 1996;334:1238–48. - PubMed
-
- Seidemann K, Tiemann M, Schrappe M, et al. Short-pulse B-non-Hodgkin lymphoma-type chemotherapy is efficacious treatment for pediatric anaplastic large cell lymphoma: a report of the Berlin-Frankfurt-Munster Group Trial NHL-BFM 90. Blood. 2001;97:3699–706. - PubMed
-
- Stein H, Mason DY, Gerdes J, et al. The expression of the Hodgkin's disease associated antigen Ki-1 in reactive and neoplastic lymphoid tissue: evidence that Reed-Sternberg cells and histiocytic malignancies are derived from activated lymphoid cells. Blood. 1985;66:848–58. - PubMed
-
- Jaffe ES, Harris NL, Stein H, Vardiman JWE. World Health Organization Classification of Tumors. Pathology and Genetics of Tumours of Haematopoietic and Lymphoid Tissues. Lyon: IARC Press; 2001.
-
- Le Deley MC, Reiter A, Williams D, et al. Prognostic factors in childhood anaplastic large cell lymphoma: results of a large European intergroup study. Blood. 2008;111:1560–6. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
