

Bariatric surgery: risks and rewards
- PMID: 18987275
- PMCID: PMC2729256
- DOI: 10.1210/jc.2008-1641
Bariatric surgery: risks and rewards
Abstract
Context: Over 23 million Americans are afflicted with severe obesity, i.e. their body mass index (in kilograms per square meter) values exceed 35. Of even greater concern is the association of the adiposity with comorbidities such as diabetes, hypertension, cardiopulmonary failure, asthma, pseudotumor cerebri, infertility, and crippling arthritis.
Objective: Diets, exercise, behavioral modification, and drugs are not effective in these individuals. This article examines the effect of surgery on the control of the weight and the comorbidities, as well as the safety of these operations.
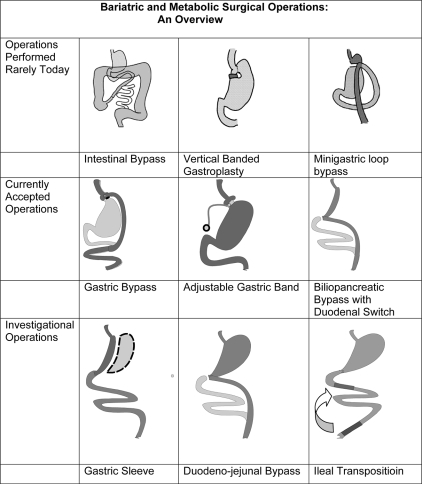
Interventions: Although the article focuses on the outcomes of the three most commonly performed operations, i.e. adjustable gastric banding, the gastric bypass, and the biliopancreatic bypass with duodenal switch, it aims for perspective with the inclusion of abandoned and current investigational procedures, a review of the complications, and an emphasis on the appropriate selection of patients. POSITIONS: Ample evidence, including controlled randomized studies, now document that bariatric surgery produces durable weight loss exceeding 100 lb (46 kg), full and long-term remission of type 2 diabetes in over 80% with salutary effects on the other comorbidities as well with significant reductions in all-cause mortality. Although the severely obese present with serious surgical risks, bariatric surgery is performed safely with a 0.35% 90-d mortality in Centers of Excellence throughout the United States-similar to the complication rates after cholecystectomy.
Conclusions: Until better approaches become available, bariatric surgery is the therapy of choice for patients with severe obesity.
Figures
References
-
- Buchwald H, Cowan, Cowan Jr GSM, Pories W 2007 Surgical management of obesity. Philadelphia: Saunders/Elsevier; 3–9
-
- Scopinaro N, Papadia F, Camerini G, Marinari G, Civalleri D, Franco AG 2008 A comparison of a personal series of biliopancreatic diversion and literature data on gastric bypass help to explain the mechanisms of resolution of type 2 diabetes by the two operations. Obes Surg 18:1035–1038 - PubMed
-
- Hess DS, Hess DW, Oakley RS 2005 The biliopancreatic diversion with the duodenal switch: results beyond 10 years. Obes Surg 15:408–416 - PubMed
-
- Rubin M, Yehoshua RT, Stein M, Lederfein D, Fichman S, Bernstine H, Eidelman LA 15 Aug 2008 Laparoscopic sleeve gastrectomy with minimal morbidity early results in 120 morbidly obese patients. Obes Surg 10.1007/s11695-008-9652-2 - PubMed
-
- Moo TA, Rubino F 2008 Gastrointestinal surgery as treatment for type 2 diabetes. Curr Opin Endocrinol Diabetes Obes 15:153–158 - PubMed
