

Immunologic, clinical, and radiologic status 14 months after cessation of natalizumab therapy
- PMID: 18987352
- PMCID: PMC2677530
- DOI: 10.1212/01.wnl.0000327341.89587.76
Immunologic, clinical, and radiologic status 14 months after cessation of natalizumab therapy
Abstract
Objective: Natalizumab is a humanized recombinant monoclonal antibody against very late activation antigen-4 approved for the treatment of patients with multiple sclerosis (MS). A phase II study failed to demonstrate a difference between natalizumab treatment groups and the placebo group with regard to gadolinium enhancing lesions on MRI 3 months after discontinuation of therapy. The objective of this study was to assess clinical MS disease activity, surrogate disease markers on MRI, immunologic parameters in peripheral blood and CSF, as well as safety in patients with MS after discontinuation of natalizumab therapy.
Methods: This study is a longitudinal and serial cross-sectional assessment, in which 23 patients who were treated with natalizumab in the context of two phase III clinical trials were originally enrolled. A subgroup of patients was followed over 14 months. The annual relapse rate, neurologic disease progression assessed by the Expanded Disability Status Scale, disease surrogate markers on MRI, cellular and humoral immune markers in peripheral blood and CSF, and adverse events of the drug were monitored.
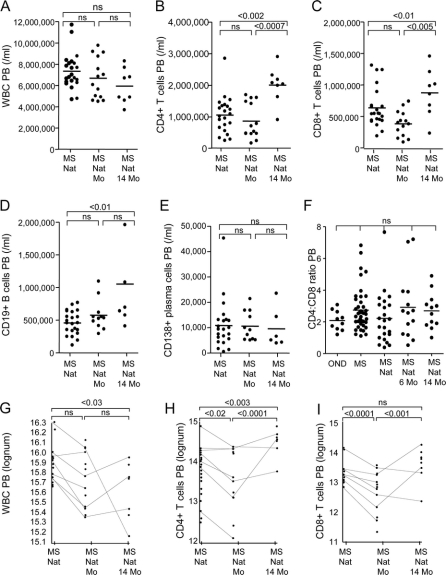
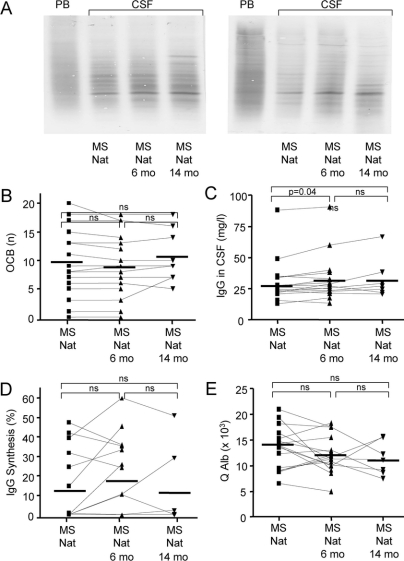
Results: With regard to clinical disease activity, neuroimaging, and immune responses, the majority of patients in our cohort were stable. Decreased lymphocyte cell numbers and altered cell ratios returned to normal 14 months after cessation of natalizumab. No infectious complications were observed.
Conclusion: This is the first long-term follow-up of patients who discontinued natalizumab. We did not observe a clinical, radiographic, or immunologic rebound phenomenon after discontinuation of natalizumab therapy.
Figures

Comment in
-
Natalizumab: bound to rebound?Neurology. 2009 Feb 3;72(5):392-3. doi: 10.1212/01.wnl.0000341783.33962.5b. Neurology. 2009. PMID: 19188569 No abstract available.
References
-
- Rudick RA, Stuart WH, Calabresi PA, et al. Natalizumab plus interferon beta-1a for relapsing multiple sclerosis. N Engl J Med 2006;354:911–923. - PubMed
-
- Polman CH, O’Connor PW, Havrdova E, et al. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med 2006;354:899–910. - PubMed
-
- Kleinschmidt-Demasters BK, Tyler KL. Progressive multifocal leukoencephalopathy complicating treatment with natalizumab and interferon beta-1a for multiple sclerosis. N Engl J Med 2005;353:369–374. - PubMed
-
- Langer-Gould A, Atlas SW, Green AJ, Bollen AW, Pelletier D. Progressive multifocal leukoencephalopathy in a patient treated with natalizumab. N Engl J Med 2005;353:375–381. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical