

Biomarkers of recovery after stroke
- PMID: 18989108
- PMCID: PMC2882885
- DOI: 10.1097/WCO.0b013e3283186f96
Biomarkers of recovery after stroke
Abstract
Purpose of review: A better understanding of the molecular events underlying stroke recovery might be useful to optimize restorative therapies. Measurement of these events, however, is generally inaccessible in humans, at least at the molecular level. Substitute measures, or biomarkers, that are accessible might provide deeper insights into spontaneous recovery in humans. This review considers advances in use of biomarkers to understand recovery from stroke, and to serve as a surrogate measure of stroke recovery, including in a clinical trial context.
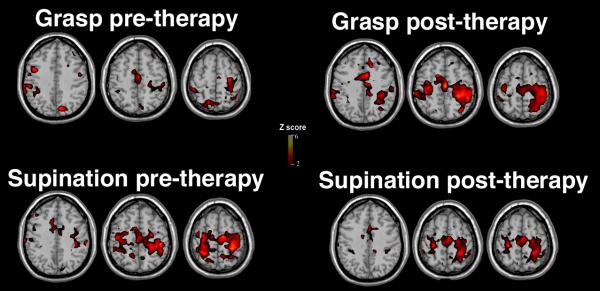
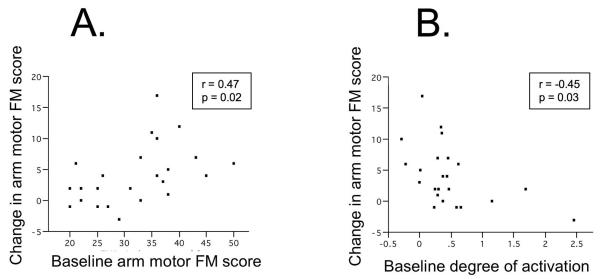
Recent findings: Among the key recent findings is that measures of brain function and injury are the strongest predictors of treatment effect, moreso than behavioral measures are, despite the reliance on behavioral measures as study entry criteria. Functional neuroimaging studies have provided insights into therapeutic mechanism of action. In addition, measures of central nervous system function have been used to estimate individual therapy needs, findings that suggest the potential to tailor restorative therapies to the specific needs of individual patients.
Summary: Many therapies are emerging as potentially useful to promote improved recovery after stroke. Continued advances in biomarkers are providing new insights into the neurobiology of both spontaneous and therapy-induced brain repair after stroke.
Figures
References
-
- Gresham G, Duncan P, Stason W, Adams H, Adelman A, Alexander D, Bishop D, Diller L, Donaldson N, Granger C, et al. Post-Stroke Rehabilitation. Rockville, MD: U.S. Department of Health and Human Services. Public Health Service, Agency for Health Care Policy and Research; 1995.
-
- Cramer SC. Repairing the human brain after stroke. II. Restorative therapies. Ann Neurol. 2008;63:549–560. - PubMed
-
- Wolf SL, Winstein CJ, Miller JP, Taub E, Uswatte G, Morris D, Giuliani C, Light KE, Nichols-Larsen D. Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke: the EXCITE randomized clinical trial. Jama. 2006;296:2095–2104. - PubMed
-
-
Wolf SL, Winstein CJ, Miller JP, Thompson PA, Taub E, Uswatte G, Morris D, Blanton S, Nichols-Larsen D, Clark PC. Retention of upper limb function in stroke survivors who have received constraint-induced movement therapy: the EXCITE randomised trial. Lancet Neurol. 2008;7:33–40. **This report provides phase 3 data showing that an intervention in patients with chronic stroke can produce significant, meaningful, and enduring behavioral gains.
-
