

Role of CCL3L1-CCR5 genotypes in the epidemic spread of HIV-1 and evaluation of vaccine efficacy
- PMID: 18989363
- PMCID: PMC2576446
- DOI: 10.1371/journal.pone.0003671
Role of CCL3L1-CCR5 genotypes in the epidemic spread of HIV-1 and evaluation of vaccine efficacy
Abstract
Background: Polymorphisms in CCR5, the major coreceptor for HIV, and CCL3L1, a potent CCR5 ligand and HIV-suppressive chemokine, are determinants of HIV-AIDS susceptibility. Here, we mathematically modeled the potential impact of these genetic factors on the epidemic spread of HIV, as well as on its prevention.
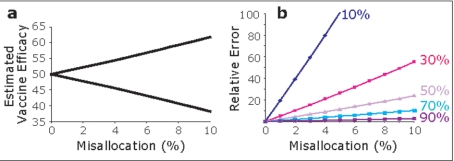
Methods and results: Ro, the basic reproductive number, is a fundamental concept in explaining the emergence and persistence of epidemics. By modeling sexual transmission among HIV+/HIV- partner pairs, we find that Ro estimates, and concordantly, the temporal and spatial patterns of HIV outgrowth are highly dependent on the infecting partners' CCL3L1-CCR5 genotype. Ro was least and highest when the infected partner possessed protective and detrimental CCL3L1-CCR5 genotypes, respectively. The modeling data indicate that in populations such as Pygmies with a high CCL3L1 gene dose and protective CCR5 genotypes, the spread of HIV might be minimal. Additionally, Pc, the critical vaccination proportion, an estimate of the fraction of the population that must be vaccinated successfully to eradicate an epidemic was <1 only when the infected partner had a protective CCL3L1-CCR5 genotype. Since in practice Pc cannot be >1, to prevent epidemic spread, population groups defined by specific CCL3L1-CCR5 genotypes might require repeated vaccination, or as our models suggest, a vaccine with an efficacy of >70%. Further, failure to account for CCL3L1-CCR5-based genetic risk might confound estimates of vaccine efficacy. For example, in a modeled trial of 500 subjects, misallocation of CCL3L1-CCR5 genotype of only 25 (5%) subjects between placebo and vaccine arms results in a relative error of approximately 12% from the true vaccine efficacy.
Conclusions: CCL3L1-CCR5 genotypes may impact on the dynamics of the HIV epidemic and, consequently, the observed heterogeneous global distribution of HIV infection. As Ro is lowest when the infecting partner has beneficial CCL3L1-CCR5 genotypes, we infer that therapeutic vaccines directed towards reducing the infectivity of the host may play a role in halting epidemic spread. Further, CCL3L1-CCR5 genotype may provide critical guidance for optimizing the design and evaluation of HIV-1 vaccine trials and prevention programs.
Conflict of interest statement
Figures



References
-
- Anderson R, Hanson M. Potential public health impact of imperfect HIV type 1 vaccines. J Infect Dis. 2005;191(Suppl 1):S85–96. - PubMed
-
- Blower S, Schwartz EJ, Mills J. Forecasting the future of HIV epidemics: the impact of antiretroviral therapies & imperfect vaccines. AIDS Rev. 2003;5:113–125. - PubMed
-
- Quinn TC, Wawer MJ, Sewankambo N, Serwadda D, Li C, et al. Viral load and heterosexual transmission of human immunodeficiency virus type 1. Rakai Project Study Group. N Engl J Med. 2000;342:921–929. - PubMed
-
- Gray RH, Wawer MJ, Brookmeyer R, Sewankambo NK, Serwadda D, et al. Probability of HIV-1 transmission per coital act in monogamous, heterosexual, HIV-1-discordant couples in Rakai, Uganda. Lancet. 2001;357:1149–1153. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
