

Case Reports
doi: 10.1109/TNSRE.2008.2003390.
Standing after spinal cord injury with four-contact nerve-cuff electrodes for quadriceps stimulation
Affiliations
- PMID: 18990650
- PMCID: PMC2936226
- DOI: 10.1109/TNSRE.2008.2003390
Item in Clipboard
Case Reports
Standing after spinal cord injury with four-contact nerve-cuff electrodes for quadriceps stimulation
IEEE Trans Neural Syst Rehabil Eng.
2008 Oct.
Abstract
This paper describes the performance of a 16-channel implanted neuroprosthesis for standing and transfers after spinal cord injury including four-contact nerve-cuff electrodes stimulating the femoral nerve for knee extension. Responses of the nerve-cuffs were stable and standing times increased by 600% over time-matched values with a similar eight-channel neuroprosthesis utilizing muscle-based electrodes on vastus lateralis for knee extension.
Figures
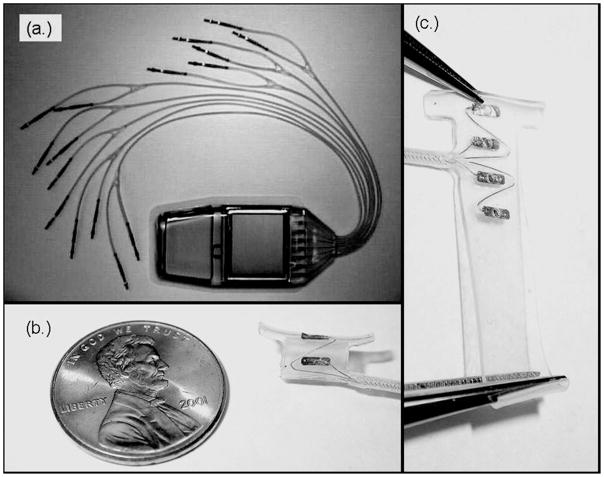
(a) The IST-16 stimulator which was implanted in a subject with SCI to restore standing function. (b) A self-sizing four-contact spiral nerve-cuff electrode used on bilateral femoral nerves in this study to stimulate the quadriceps muscles for knee extension. (c) The unspiraled nerve-cuff. All four contacts and the lead wire are visible.

Average threshold charge injected and standard deviation on all four contacts of both right and left nerve-cuff electrodes.

Peak isokinetic extension moment for left and right knees at 16 weeks post-implantation. Averaged data and standard deviations are shown for epimysial electrodes on VL in the IRS-8 system as well as for nerve-cuff electrodes on the femoral nerve in the IST-16 system. Data for individual and combinations of nerve-cuff contacts that isolated the vasti are shown.
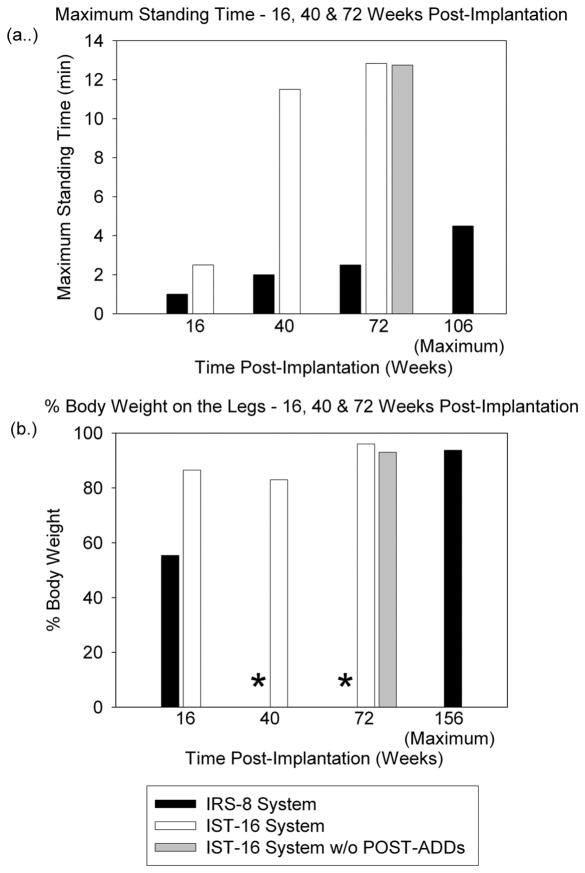
(a) Maximum standing time and (b) %BW on the legs at 16, 40, and 72 weeks post-implantation. Data are shown for the IRS-8 system, the complete IST-16 system, and the IST-16 system without stimulation of the POST-ADDs. Maximal values achieved with the epimysial IRS-8 system are presented for comparison. %BW data for 40 and 72 weeks post-implantation with the IRS-8 system (*) were unavailable.
References
-
- Jaeger R, Yarkony G, Smith R. Standing the spinal cord injured patient by electrical stimulation: Refinement of a protocol for clinical use. IEEE Trans Biomed Eng. 1989;36:720–728. - PubMed
-
- Kralj A, Bajd T. Functional Electrical Stimulation: Standing and Walking After Spinal Cord Injury. Boca Raton: CRC Press; 1989.
-
- Davis JA, Triolo RJ, Uhlir JP, Bieri C, Rohde L, Lissy D. Preliminary Performance of a surgically implanted neuroprosthesis for standing and transfers – Where do we stand? J Rehabil Res Dev. 2001;38(6):609–617. - PubMed
-
- Davis JA, Triolo RJ, Uhlir JP, Bhadra N, Lissy DA, Nandurkar S, Marsolais EB. Surgical technique for installing an 8-channel neuroprosthesis for standing. Clin Orthop Relat Res. 2001;4:237–252. - PubMed
-
- Triolo RJ, Bieri C, Uhlir J, Kobetic R, Scheiner A, Marsolais EB. Implanted FNS systems for assisted standing and transfers for individuals with cervical spinal cord injuries: clinical case reports. Arch Phys Med Rehabil. 1996;77(11):1119–1128. - PubMed
