

Self-report versus medical records for assessing cancer-preventive services delivery
- PMID: 18990740
- PMCID: PMC2962564
- DOI: 10.1158/1055-9965.EPI-08-0177
Self-report versus medical records for assessing cancer-preventive services delivery
Abstract
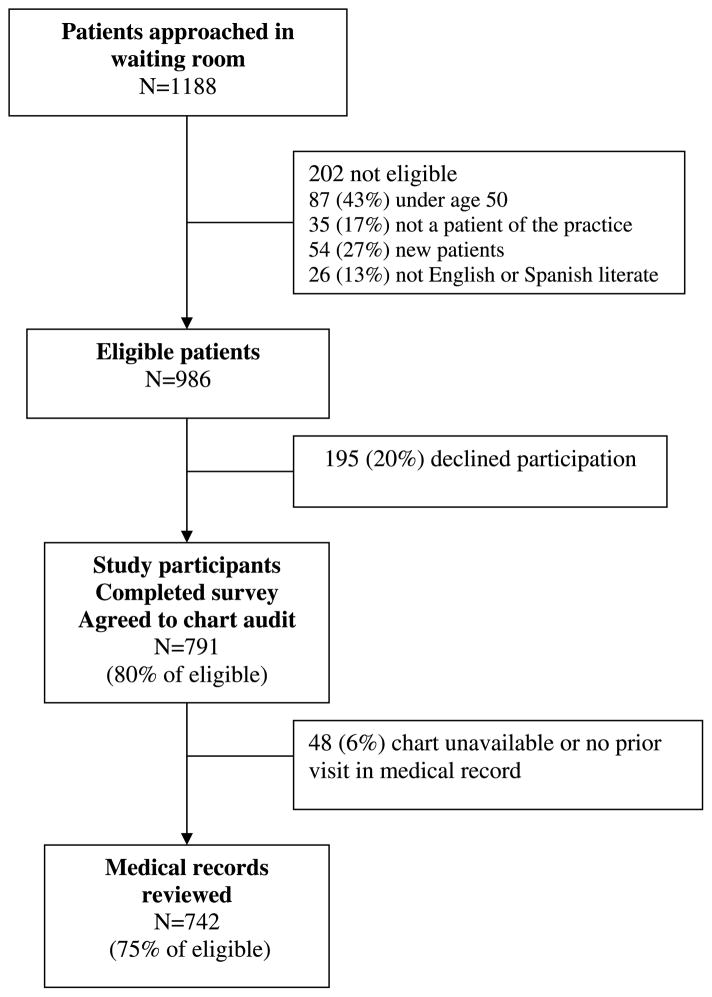
Accurate measurement of cancer-preventive behaviors is important for quality improvement, research studies, and public health surveillance. Findings differ, however, depending on whether patient self-report or medical records are used as the data source. We evaluated concordance between patient self-report and medical records on risk factors, cancer screening, and behavioral counseling among primary care patients. Data from patient surveys and medical records were compared from 742 patients in 25 New Jersey primary care practices participating at baseline in SCOPE (supporting colorectal cancer outcomes through participatory enhancements), an intervention trial to improve colorectal cancer screening in primary care offices. Sensitivity, specificity, and rates of agreement describe concordance between self-report and medical records for risk factors (personal or family history of cancer, smoking), cancer screening (breast, cervical, colorectal, prostate), and counseling (cancer screening recommendations, diet or weight loss, exercise, smoking cessation). Rates of agreement ranged from 41% (smoking cessation counseling) to 96% (personal history of cancer). Cancer screening agreement ranged from 61% (Pap and prostate-specific antigen) to 83% (colorectal endoscopy) with self-report rates greater than medical record rates. Counseling was also reported more frequently by self-report (83% by patient self-report versus 34% by medical record for smoking cessation counseling). Deciding which data source to use will depend on the outcome of interest, whether the data is used for clinical decision making, performance tracking, or population surveillance; the availability of resources; and whether a false positive or a false negative is of more concern.
Conflict of interest statement
No potential conflicts of interest were disclosed.
References
-
- Schenck AP, Klabunde CN, Warren JL, et al. Data sources for measuring colorectal endoscopy use among Medicare enrollees. Cancer Epidemiol Biomarkers Prev. 2007;16:2118–27. - PubMed
-
- Beckles GL, Williamson DF, Brown AF, et al. Agreement between self-reports and medical records was only fair in a cross-sectional study of performance of annual eye examinations among adults with diabetes in managed care. Med Care. 2007;45:876–83. - PubMed
-
- Newell SA, Girgis A, Sanson-Fisher RW, et al. The accuracy of self-reported health behaviors and risk factors relating to cancer and cardiovascular disease in the general population: a critical review. Am J Prev Med. 1999;17:211–29. - PubMed
-
- Tisnado DM, Adams JL, Liu H, et al. What is the concordance between the medical record and patient self-report as data sources for ambulatory care? Med Care. 2006;44:132–40. - PubMed
-
- Tisnado DM, Adams JL, Liu H, et al. Does concordance between data sources vary by medical organization type? Am J Manag Care. 2007;13:289–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
